|
My intent in redesigning this page is to break
out the health care reform issue into topic
areas, i.e., PPACA (the Patient
Protection and Affordable Care Act); covering
the uninsured and universal health care;
quality; costs; and specific reforms like
managing managed care, accounting for care,
rationing care, and the like, and to sort the
resources and discussion into topic areas for
easier retrieval.
contents
Patient Protection
and Affordable Care Act
Let Sleeping Gorillas Lie: Setting the Benefit Rules Under PPACA
Quality Matters
Where Does the United States REALLY Rank Among
Nations When it Comes to Health Care?
Does the U.S. have too few physicians, or too few primary care
practitioners?
Cost Controls
Everything You Ever Wanted to Know About the
PPACA Independent Payment Advisory Board But
Were Afraid to Ask
Buried in PPACA (Obamacare) is a secret weapon
to contain Medicare costs... the IPAB. Meet
the group of House Democrats who want to
destroy it.
 The Independent Payment Advisory Board Under Fire: Can Its Opponents
Succeed in Killing It? The Independent Payment Advisory Board Under Fire: Can Its Opponents
Succeed in Killing It?
Payment Changes and
Reforms
Everything You Ever Wanted to Know About the
PPACA Independent Payment Advisory Board But
Were Afraid to Ask
Financing Changes,
Taxes and Premiums
Means-Testing Medicare: The rich have been
getting richer. Should they should pay more? Or
get less?
The Budgetary Impact of the New Health Care
Reform Law Over 10 Years and Beyond
Health Care is Now 17.6% of the Nation's
Gross Domestic Product
U.S. Taxpayers are
Over-Taxed... Not! ...(when compared to
other industrialized nations; we're just not
getting what we pay for)...
PPACA
Truths, Lies and Distortions
The Biggest and Baddest Lies about PPACA
("Obamacare")
Is PPACA a "Job-Killing, Budget-Busting Law?"
Not According to the Facts.
Repeal of PPACA is the REAL Job-Busting
Action
Covering the
Uninsured and Underinsured
 Mini-Med ... and the Underinsured Mini-Med ... and the Underinsured
Let's Just Allow
the Buying of Health Insurance Across State
Lines, That's the Ticket, Cheaper Insurance...
NOT! Another Failed TeaParty/GOP Idea
Insurance Across State Lines: Sounds
Good... on Paper ... But Consider the
Real Impact ... And Besides it Does NOTHING to
Solve Insurance Affordability and at Best Might
Get Another 4 Million Insured... A Drop in the
Bucket
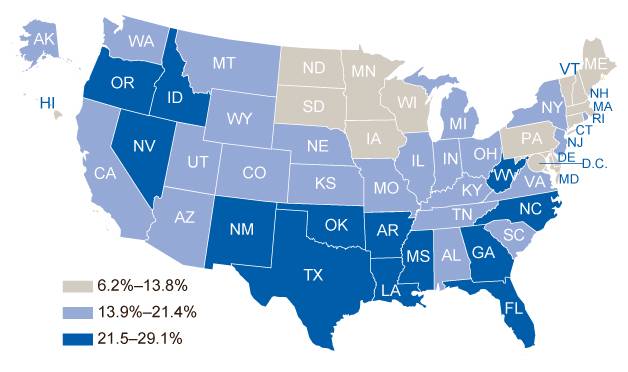
The Nation's Uninsured (as seen by the Centers for Disease Control)
Gosh Darn All
Those Pesky Uninsured People...
Rationing
Let's Kill Granny! Health Care Rationing For Me
But Mostly You...
Changing How Health
Care is Delivered
Too Many Doctors? Too Few Nurses!
Taming the Unicorn: Accounting for Accountable
Care Organizations (ACOs)
ACCOUNTABLE CARE ORGANIZATIONS: New Rules
Soon... Very Soon
... and after
reviewing any of these "thoughts," you are
offended or challenged... or maybe you just want
to go into it a bit more, drop Jeanne an e-mail
and open the dialog:
jeanne.matthews@health-politics.
... and things only tangentially-related to
health care ...
The Pope hates nuns because ...

Where Does the United States REALLY Rank Among
Nations When it Comes to Health Care?
The famous (or is it infamous) World
Health Organization survey of 1998-99, ranked the United States 37th
in the world when it came to the overall effectiveness of its health
care system, just two places ahead of Cuba and one behind Costa Rica
(see chart below)
|
1 France |
66 Hungary |
131 Honduras |
|
2 Italy |
67 Trinidad and Tobago |
132 Burkina Faso |
|
3 San Marino |
68 Saint Lucia |
133 Sao Tome and Principe |
|
4 Andorra |
69 Belize |
134 Sudan |
|
5 Malta |
70 Turkey |
135 Ghana |
|
6 Singapore |
71 Nicaragua |
136 Tuvalu |
|
7 Spain |
72 Belarus |
137 Ivory Coast |
|
8 Oman |
73 Lithuania |
138 Haiti |
|
9 Austria |
74 St. Vincent- Grenadines |
139 Gabon |
|
10 Japan |
75 Argentina |
140 Kenya |
|
11 Norway |
76 Sri Lanka |
141 Marshall Islands |
|
12 Portugal |
77 Estonia |
142 Kiribati |
|
13 Monaco |
78 Guatemala |
143 Burundi |
|
14 Greece |
79 Ukraine |
144 China |
|
15 Iceland |
80 Solomon Islands |
145 Mongolia |
|
16 Luxembourg |
81 Algeria |
146 Gambia |
|
17 Netherlands |
82 Palau |
147 Maldives |
|
18 United Kingdom |
83 Jordan |
148 Papua New Guinea |
|
19 Ireland |
84 Mauritius |
149 Uganda |
|
20 Switzerland |
85 Grenada |
150 Nepal |
|
21 Belgium |
86 Antigua-Barbuda |
151 Kyrgystan |
|
22 Colombia |
87 Libya |
152 Togo |
|
23 Sweden |
88 Bangladesh |
153 Turkmenistan |
|
24 Cyprus |
89 Macedonia |
154 Tajikistan |
|
25 Germany |
90 Bosnia-Herzegovina |
155 Zimbabwe |
|
26 Saudi Arabia |
91 Lebanon |
156 Tanzania |
|
27 United Arab Emirates |
92 Indonesia |
157 Djibouti |
|
28 Israel |
93 Iran |
158 Eritrea |
|
29 Morocco |
94 Bahamas |
159 Madagascar |
|
30 Canada |
95 Panama |
160 Vietnam |
|
31 Finland |
96 Fiji |
161 Guinea |
|
32 Australia |
97 Benin |
162 Mauritania |
|
33 Chile |
98 Nauru |
163 Mali |
|
34 Denmark |
99 Romania |
164 Cameroon |
|
35 Dominica |
100 Saint Kitts & Nevis |
165 Laos |
|
36 Costa Rica |
101 Moldova |
166 Congo |
|
37
United States of America |
102 Bulgaria |
167 North Korea |
|
38 Slovenia |
103 Iraq |
168 Namibia |
|
39 Cuba |
104 Armenia |
169 Botswana |
|
40 Brunei |
105 Latvia |
170 Niger |
|
41 New Zealand |
106 Yugoslavia |
171 Equatorial Guinea |
|
42 Bahrain |
107 Cook Islands |
172 Rwanda |
|
43 Croatia |
108 Syria |
173 Afghanistan |
|
44 Qatar |
109 Azerbaijan |
174 Cambodia |
|
45 Kuwait |
110 Suriname |
175 South Africa |
|
46 Barbados |
111 Ecuador |
176 Guinea-Bissau |
|
47 Thailand |
112 India |
177 Swaziland |
|
48 Czech Republic |
113 Cape Verde |
178 Chad |
|
49 Malaysia |
114 Georgia |
179 Somalia |
|
50 Poland |
115 El Salvador |
180 Ethiopia |
|
51 Dominican Republic |
116 Tonga |
181 Angola |
|
52 Tunisia |
117 Uzbekistan |
182 Zambia |
|
53 Jamaica |
118 Comoros |
183 Lesotho |
|
54 Venezuela |
119 Samoa |
184 Mozambique |
|
55 Albania |
120 Yemen |
185 Malawi |
|
56 Seychelles |
121 Niue |
186 Liberia |
|
57 Paraguay |
122 Pakistan |
187 Nigeria |
|
58 South Korea |
123 Micronesia |
188 Dem. Rep. of Congo |
|
59 Senegal |
124 Bhutan |
189 Cent. African Republic |
|
60 Philippines |
125 Brazil |
190 Myanmar |
|
61 Mexico |
126 Bolivia |
|
|
62 Slovakia |
127 Vanuatu |
|
|
63 Egypt |
128 Guyana |
|
|
64 Kazakhstan |
129 Peru |
|
|
65 Uruguay |
130 Russia |
|
And while the survey upon which these
rankings were give is now more than a dozen years old ... and subject
to considerable crit icism
and debate. it is still the one most commonly cited by most media
outlets and so-called health care gurus, including such celebrities as
Michael Moore in his award-winning documentary, "SiCKO." Another
such guru, one Jeanne Scott Matthews, has (in the past) used these
rankings often in her writings and presentations. But it is time to
admit that this survey and these rankings are
no longer meaningful and have become deceptive in both use
during the health care debate and in drawing any conclusions about the
U.S. health care system.
I hereby pledge to nevermore use this chart or these numbers. icism
and debate. it is still the one most commonly cited by most media
outlets and so-called health care gurus, including such celebrities as
Michael Moore in his award-winning documentary, "SiCKO." Another
such guru, one Jeanne Scott Matthews, has (in the past) used these
rankings often in her writings and presentations. But it is time to
admit that this survey and these rankings are
no longer meaningful and have become deceptive in both use
during the health care debate and in drawing any conclusions about the
U.S. health care system.
I hereby pledge to nevermore use this chart or these numbers.
So how can we to evaluate the quality,
effectiveness and standing of U.S. health care in relation to the rest
of the world, and in particular to other industrialized nations with
whom we compete economically in world markets?
How much we spend and what we are getting in
return for our money are increasingly important measures impacting
this nation's future competitiveness and will play a critical part in
resolving our country's economic woes and budgetary problems.
One thing we cannot do, is stay in place and do nothing.
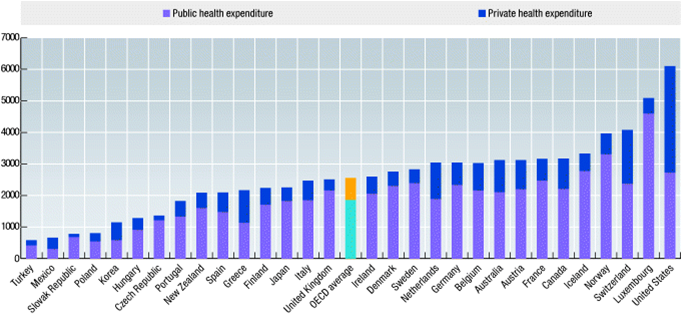
There are a number of newer... and
apparently more reliable surveys to be considered. One is the regular
rankings from the Organisation for Economic Cooperation and
Development (OECD)
|
The Organisation for European Economic Cooperation (OEEC) was
established in 1947 to run the US-financed Marshall Plan for
reconstruction of a continent ravaged by war. By making individual
governments recognise the interdependence of their economies, it
paved the way for a new era of cooperation that was to change the
face of Europe. Encouraged by its success and the prospect of
carrying its work forward on a global stage, Canada and the US
joined OEEC members in signing the new OECD Convention on 14
December 1960.
The Organisation for Economic Co-operation and Development
(OECD) was officially born on 30 September 1961, when the
Convention entered into force. Other countries joined in,
starting with Japan in 1964. Today, 34 OECD member countries
worldwide regularly turn to one another to identify problems,
discuss and analyse them, and promote policies to solve them. The
track record is striking. The US has seen its national wealth
almost triple in the five decades since the OECD was created,
calculated in terms of gross domestic product per head of
population. Other OECD countries have seen similar, and in some
cases even more spectacular, progress.
So, too, have countries that a few decades ago were still only
minor players on the world stage. China, India and Brazil have
emerged as new economic giants. Most of the countries that formed
part of the former Soviet bloc have either joined the OECD or
adopted its standards and principles to achieve our common goals.
Russia is negotiating to become a member of the OECD, and we now
have close relations with Brazil, China, India, Indonesia and
South Africa through our enhanced engagement programme. Together
with them, the OECD brings around its table 40 countries that
account for 80% of world trade and investment, giving it a pivotal
role in addressing the challenges facing the world economy. |
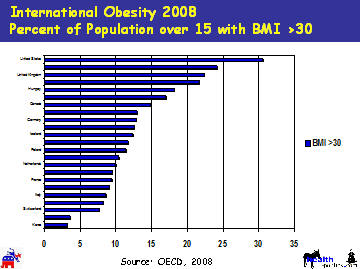
According to the OECD. the United States
ranks well down the list of the 34 counties in virtually every health
indicator category... well except for a couple.
We spend more per capita than any other
OECD country, by a lot:
Americans are more obese on average than
people in other OECD countries. (For the record, I contribute more
than my fair share to this record):

But there is one, new and VERY interesting ranking,
this from the Gallup people, and using "survey" results obtained from
"in person" interviews using standard statistical and polling
mechanisms. While "polling" is still not an exact science, its
methodologies have improved significantly. The Gallup people have also
introduced some "touchy-feely" aspects to their rating system...
"thriving," "struggling," "suffering," In this survey the
U.S. ranks considerably higher but still lags all of the Scandinavian
countries and our English-speaking "sister" British-descendant
nations, Australia, New Zealand and Canada, but ahead of continental
Europe.
Gallup Global Wellbeing Index by Country 2010
Countries Ranked by % Thriving
Gallups global wellbeing metrics are the first comprehensive
measure of the behavioral economics of gross national wellbeing, which
lays the foundation for all other measures of a countrys economic
strength. With ongoing research projects in more than 150 countries,
Gallup is a leader in the collection and analysis of global data and
measurements.
Gallup asks ordinary individuals for their thoughts and opinions on
several topics, including economics, religion, migration, and
wellbeing. Gallups data provide sound evidence on many issues that
more than 98% of the worlds adult population faces.
The table shows life evaluation estimates of the percentage
thriving, struggling, and suffering in countries and regions
across the world. Gallups Thriving, Struggling, and Suffering indexes
measure respondents perceptions of where they stand now and in the
future. Based on the Cantril Self-Anchoring Striving Scale, Gallup
measures life satisfaction by asking respondents to rate their present
and future lives on a ladder scale with steps numbered from 0 to 10,
where 0 indicates the worst possible life and 10 the best possible
life. Individuals who rate their current lives a 7 or higher and
their future an 8 or higher are considered thriving. Individuals are
suffering if they report their current and future lives as a 4 or
lower. All other individuals are considered struggling.
The table also includes daily wellbeing averages (0-10 scoring) based
on responses to 10 items measuring daily experiences (feeling
well-rested, being treated with respect, smiling/laughter,
learning/interest, enjoyment, physical pain, worry, sadness, stress,
and anger). Each daily experience is scored dichotomously with higher
scores representing better days (more positive and less negative daily
experience or affect).
*Limited urban samples only.
Means-Testing Medicare: The rich have been
getting richer. Should they should pay more? Or
get less?
One of the more recent phenomenons of my advanced years has been how
readily (and easily) I may change some of my most intense and deeply
held political beliefs. Ive already cited my change in philosophy
regarding the
percent
of GDP spent on health care; now I am re-visiting Medicare
means-testing. Its kind of like that old Samuel Clemens/Mark
Twain adage, When I was young, my father was the most stubborn,
mule-headed, son-of-a-bitch, I had ever seen. But now that I am older,
its amazing how much smarter he has gotten. But in my
case, my personal mule-headedness may only date to my 50s, and my
smarter(ness) seems to have come in my late 60s. <sigh>
Back before the turn of the century, I wrote (and spoke regularly)
about the issue of means-testing Medicare, rejecting the concept as a
sell-out to the original egalitarian principles of both Medicare and
its big sister, Social Security. These two benefit programs had
become an integral part of the
social contract that bound the
nation together. Every citizen who met the minimum qualifications
would be eligible; the bag-lady who sleeps over the grating outside
Union Station in Washington DC would get them, Bill Gates would get
them. The programs were completely egalitarian.
Way, way back in April 1999, in my regular monthly column in the Journal of the
Healthcare Financial Management Association, I wrote about,
"Changing the Medicare Social Contract" I first began to
discuss the potential for "means-testing Medicare. Back then, the
driving issue was a GOP-majority report
from
one of the seemingly unlimited Medicare commissions that suggested
something labeled: premium support.
Under a
premium support model, Medicare would credit each eligible beneficiary
with an equal allocation, an amount currently estimated to be 88
percent of the average per capita amount Medicare spends. Based on the
then available 1998 expenditures, this amount would have been
approximately $4,994 (88 percent of the $5,675 a year HCFA (now CM2)
then said it was paying per beneficiary for Part A and Part B
Medicare). Future Medicare allocations would have been adjusted yearly
based on actual expenditures and budgetary decisions. Premium
support advocates (mostly Republican) were seeking to "penalize" those
who might choose a more expensive plan by reducing their 88 percent
allocation while raising the allocation for lower-income individuals.
In effect, under the plan, Medicare beneficiaries would be subject to
means testing, thus transforming Medicare into a multitiered social
benefits program with all of the trappings of a full-fledged welfare
program.
Welfarizing Medicare (and Social
Security)
Now welfare-like provisions have been creeping into
Medicare and Social Security for some time. We have begun taxing the
Social Security benefits of retirees with retirement incomes greater
than $35,000 a year - in effect, taking back from the "wealthy" some
of their "entitlement" to the full benefits of that program.
Similarly, under Medicare, by subjecting every dollar of income to the
Medicare tax with no increase in benefits, the wealthier have been
paying more for their coverage for the past several years and
effectively subsidizing poorer people who pay less. In 2003, with the
passage of the Medicare Modernization Act (the law that gave us
Medicare Part D, prescription drugs) we began the most direct
means-testing of Medicare, increasing the monthly Medicare Part B
premium for those with incomes over $80,000 a year. At the time
Democrats were unalterably opposed to this, holding fast to
their egalitarian views. The prescription drug benefit provisions in
the 2003 MMA (I prefer the acronym "NAIM")
got all the attention but other changes to Medicare may end up having
far more long term impact... mostly specifically the establishment of
new Medicare Part C, the 2003 version of "premium support." For the
first time, we tiered Medicare directly, with wealthier individuals
paying higher monthly premiums, ranging from 20% to 100% more, on a
rising scale.
Democrats went postal at the time and the new law was
passed without a single Democratic vote. The Democrats fought the
"welfarization" of Medicare, fearing that in the long term, as merely
another "welfare" program, the entitlement nature of the program would
change forever, and with it, as the tides of time and change moved,
would public support for the program.
But I am not the only one getting smarter in my old
age, by 2010, in PPACA, Democrats had come virtually full circle on
the means-testing issue and almost eagerly added a means test of their
own, extending the GOP-driven rising scale of premiums for Medicare
Part B to Medicare Part D. Will Medicare Part A be next?
As an interesting side fact, a survey showed that by
2008, that Democrats favored means-testing Medicare at a statistically
higher rate than Republicans. You can draw your own conclusions about
that, but egalitarian attitudes toward Medicare (and,
presumably Social Security, would be appear to have died a slow and
apparently not too painful Democratic mind-set death.
Changing the Social Contract
 The
egalitarian philosophy that was so much a part of Medicare in the
beginning - that all Americans are entitled to receive Medicare simply
because they are Americans -- is breaking down. Not that there's
anything wrong with that. Social contracts can be changed as long as
the American electorate understands and agrees to the change. But
therein lies a very irritating rub, the Social Contract, is being
changed secretly, incrementally without the understanding "advice and
consent" of the people. The
egalitarian philosophy that was so much a part of Medicare in the
beginning - that all Americans are entitled to receive Medicare simply
because they are Americans -- is breaking down. Not that there's
anything wrong with that. Social contracts can be changed as long as
the American electorate understands and agrees to the change. But
therein lies a very irritating rub, the Social Contract, is being
changed secretly, incrementally without the understanding "advice and
consent" of the people.
The idea of "privatizing" Medicare as pushed by
today's TeaParty/GOPers should be a non-starter. They would
essentially gut the entire program (albeit, as explained me by one of
the "pool people" in my senior 55+ community in Arizona, "I know it
would ultimately destroy Medicare, but it'll take them years to
implement. By then I will be gone and won't worry about it.) She is an
enthusiastic TeaParty/GOPer. But we do need to look at ways where
means-testing may benefit not just the low to middle income
beneficiaries of today, but those of tomorrow as well. We do need to
couple any such mans-testing with major payment reforms and delivery
changes. Gosh for an old lady, I have a lot of work to do.
back to
top
Is PPACA a "Job-Killing, Budget-Busting Law?"
Not According to the Facts.
 When
it comes to truth in labeling, House
Republicans are getting off to a poor start
with their constantly repeated references to
the new health care law as "job-killing." When
it comes to truth in labeling, House
Republicans are getting off to a poor start
with their constantly repeated references to
the new health care law as "job-killing."
The Facts:
-
Independent, nonpartisan experts
project only a "small" or "minimal" impact on
jobs, even before taking likely job gains in
the health care and insurance industries into
account.
-
The House Republican leadership,
in a report issued January 6, badly
misrepresents what the Congressional Budget
Office has said about the law. In fact, CBO is
among those saying the effect "will probably
be small."
-
The GOP also cites a study
projecting a 1.6 million job loss but fails
to mention that the study refers to a
hypothetical employer mandate that is not part
of the new law.
-
The same study cited by the GOP
also predicts an offsetting gain of 890,000
jobs in hospitals, doctors offices and
insurance companies a factor not mentioned
by the House leadership.
Theres little doubt that the new
law will likely lead to somewhat fewer low-wage
jobs. Thats mainly because of the laws
requirement that, generally, firms with more
than 50 workers pay a penalty if they fail to
provide health coverage for their workers. One
leading health care expert, John Sheils of The
Lewin Group, puts the loss at between 150,000
and 300,000 jobs, at or near the minimum wage.
And Sheils says that relatively small loss would
be partly offset by gains in the health care
industry.
Analysis
Attaching misleading labels to
legislation is a well-worn tactic in
Washington. Conservatives got rid of most of
the estate tax after labeling it a "death
tax," as though it taxed death instead of
multimillion-dollar fortunes. And liberals
once won passage of an "assault weapons ban"
that didnt really ban fully automatic
military assault rifles, which were already
illegal for civilians to own without a
very-hard-to-get federal license. Now House
Republicans are seeking to repeal what they
call "Obamacare:
A budget-busting, job-killing health care
law." Thats the title of a study issued
by the House Republican leadership
January 6.
And the GOP is clearly pushing the
"job-killer" claim. House Speaker John Boehner
used the phrase "job-killing" to describe the
health care law seven times on Thursday in
a press conference that lasted less than 14
minutes thats once every 2 minutes. He also
used the phrases "destroy jobs" and "destroying
jobs" once each when talking about the law.
Perhaps not surprisingly, the Republicans named
their
bill to repeal the health care law:
"Repealing the Job-Killing Health Care Law Act."
But is the
health care law really "job-killing" as claimed?
That's just another case of exaggerated and
misleading labeling.
Job-Killing?
To support
its claim, the GOP report first cites the
nonpartisan Congressional Budget Office but
the report badly misrepresents what CBO actually
said.
House GOP Leadership, January 6: The
health care law will cause significant job
losses for the U.S. economy: the Congressional
Budget Office has determined that the law will
reduce the amount of labor used in the
economy by
roughly half a percent
, an
estimate that adds up to roughly 650,000 jobs
lost.
In fact,
CBO did not predict a 650,000 job loss. The
Republican report cites
a CBO report from August, which actually
said that the economy will use less labor
primarily because many people will choose to
work less, or retire early, as a result of the
new law. What CBO projects is mostly a
reduction in the supply of labor, which is not
the same as a reduction in the supply of jobs.
CBO, August 2010: The Congressional
Budget Office (CBO) estimates that the
legislation, on net, will reduce the amount of
labor used in the economy by a small
amountroughly half a percentprimarily
by reducing the amount of labor that workers
choose to supply.
CBO said
one reason fewer people will choose to work is
that many low-income people will have more money
in their pockets as a result of the law
expanding Medicaid and providing federal
subsidies for many who buy insurance privately.
"The expansion of Medicaid and the availability
of subsidies through the exchanges will
effectively increase beneficiaries financial
resources," CBO said. "Those additional
resources will encourage some people to work
fewer hours or to withdraw from the labor
market."
Another
reason that people might work less is that the
new law requires insurance companies to cover
preexisting conditions, and also limits their
ability to charge higher rates for older persons
who buy policies for themselves. "As a result,
some older workers will choose to retire earlier
than they otherwise would," CBO said.
To be
sure, some jobs will indeed be lost, CBO said.
Thats because the new law requires many
businesses to pay a penalty if they do not
provide health insurance to their workers. That
"will probably cause some employers to respond
by hiring fewer low-wage workers," CBO said. But
it also said these firms may hire more part-time
or seasonal workers instead. CBO did not
estimate the number of jobs likely to be
affected either way.
In a more
extensive look at the subject,
CBO on July 14, 2009, said the effect of the
employer mandate "would probably be small."
The GOP report did not mention that.
Finally,
CBO did not attempt to estimate the number of
jobs likely to be gained in the health care and
insurance industries. It has projected that the
law will result in 32 million Americans gaining
health insurance that they would not otherwise
have, enabling them to buy more services from
physicians and other health care providers. More
about that later.
Others Estimate Small, Minimal Impact
The Lewin
Group also has estimated a small impact on jobs
as a result of the health care law. Senior Vice
President John Sheils said Lewins analysis
showed 150,000 to 300,000 jobs lost, all minimum
wage or near minimum wage positions that would
be lost permanently. That doesnt account for
increases in jobs in other sectors, mainly
health care, that Sheils also expects but hasnt
quantified. All told, he estimates, a "small net
job loss."
(TRUTH-IN-REPORTING: Lewin is a subsidiary of
UnitedHealth Group, a
huge for-profit health insurer) The reason
that some low-wage workers are expected to lose
jobs, as CBO also said, is that some employers
who are faced with penalties will pass along
those costs to workers in the form of lower
wages or reduced benefits. For low-wage workers,
their wages cant be reduced below the minimum
wage, so those firms would hire less, lay off
workers or use more part-time employment.
Sheils notes that there will be
distributional effects, as some sectors gain
jobs and others lose them, but the people
gaining employment arent necessarily the same
who lost jobs. He says theres "a potentially
painful process here in changes in employment in
some industries
versus others." Skilled
workers are likely to benefit.In Nov 2009 the
House was debating a health care bill with
tougher requirements and penalties for employers
than the law now has. Even under that bill,
Elizabeth McGlynn, associate director of the
health unit at RAND Corp., told us the effect on
jobs "is likely to be quite minimal." McGlynn
said: "Most large businesses already offer
health insurance. And most small businesses are
excluded from the mandate. So its relatively
few firms that will be affected."
And small
businesses those with 50 or fewer employees
are likely to benefit under the law, Sheils
says. "I think they actually could come out
ahead," he says. "They dont face the mandate
and they could get a tax credit at least for a
while for their health benefit.
It gives them
an advantage in the marketplace," if theyre
competing against larger firms.
Besides Sheils numbers and CBOs
estimate, no other nonpartisan figures on the
laws impact on jobs have been found. When
Sheils was
asked if he knew of others, he said
no. He added that he thinks that a lot of
economists believe the effect is small, and
thats why theyre not doing an analysis.
1.6 million lost jobs?
The second
piece of evidence offered by the GOP report is a
study by the National Federation of Independent
Business, projecting a 1.6 million job loss. But
here the GOP misrepresents the evidence again.
The NFIB did not study the new law. Its report
was based on a hypothetical employer mandate
that bears little resemblance to what was
actually passed and it also projects a gain of
hundreds of thousands of health care and
insurance industry jobs.
House GOP Leadership, January 6: A
study by the National Federation of
Independent Businesses (NFIB), the nations
largest small business association, found that
an employer mandate alone could lead to the
elimination of 1.6 million jobs between 2009
and 2014, with 66 percent of those coming from
small businesses.
That
refers to
a study by the NFIBs Research Foundation.
But that study was issued
January 26, 2009 well over a year
before the new law was actually enacted. NFIB
has not issued any study of what actually became
law, and one of this studys authors, Michael
Chow, told us by e-mail that it has no present
plans to do so.
The GOP
report refers to the NFIBs analysis as
"independent," but its hardly a neutral source.
The federation is
currently backing repeal of the new law, and
has historically been opposed to any requirement
that businesses provide coverage for their
workers. NFIB also
cosponsored with the Chamber of Commerce an
ad criticizing health care legislation in 2009.
More
important, what the NFIB foundation studied was
not what became law. It gave its estimate of the
effect of a hypothetical employer mandate that
would cover all businesses, and require that
they pay at least half the insurance premiums
for their workers.
NFIB Research Foundation, January 26, 2009:
[T]he employer mandate would cause the economy
to lose over 1.6 million jobs within the first
five years of program implementation. Small
firms would be most adversely affected by the
mandate and account for approximately 66
percent of all jobs lost.
Even if
that 1.6 million figure were accurate, it
wouldnt apply to the new law that was signed
last March. The
new law does not require all businesses to
provide coverage. It exempts those with 50 or
fewer workers. So the "small firms" that the
NFIB study says would be "most adversely
affected" by the imaginary mandate studied in
2009 will not be affected at all by the actual
law. The 1.6 million figure is a gross
exaggeration of the likely effect of the law,
even using the NFIBs study as a guide.
Looking
closely at the study. Its not possible to say
precisely how big a job loss it would have
predicted had the 50-worker exemption been
factored in. It predicts that the mandate would
cause 467,182 jobs to be lost in firms employing
19 or fewer workers, so the 1.6 million figure
is high by at least that much. (See Table 6,
page 17.) In addition, the study estimates that
420,600 jobs would be lost in firms employing
from 20 to 99 workers, so some large but unknown
share of those would also have to be subtracted,
possibly reducing the figure to 1 million or
less.
And
although neither the NFIB nor the GOP leadership
report mentions it, this is a gross figure, not
a net figure. It fails to account for job gains
brought about by the new law, a point already
mentioned. And buried deep in the NFIBs own
report is evidence that those job gains could be
substantial.
890,000 New Jobs?
Heres
what the NFIB report said about job gains, on
page 20:
NFIB Research Foundation, January 26, 2009:
The employer mandate would boost demand for
healthcare goods and services, thereby
increasing employment in healthcare-related
sectors. The number of ambulatory healthcare
professionals (physicians, dentists, and other
healthcare practitioners) needed will increase
by 330,000. An additional 327,000 staff will
be required to work in hospitals. Some 157,000
more nurses (net of retirements) will be
needed to staff doctors offices, outpatient
clinics, and other provider locations. And
payrolls at insurance companies will expand by
76,000 workers.
That comes
to 890,000 new jobs.
Although
the new law relies more on an individual mandate
requiring nearly everybody to obtain coverage
on their own if their employers dont provide it
the resulting increase in demand for health
care services, prescription drugs and other
goods would be the same. To repeat, CBO
estimates that the law will result in 32 million
additional persons with health coverage.
The NFIB
study cautioned that some of those 890,000 new
jobs might not be filled right away if the
increased demand outstrips the health care
systems ability to meet it. But even so, it
amounts to a sizeable offset to the jobs likely
to be lost due to the employer mandate.
For the
record, conservatives arent the only ones
misrepresenting the laws likely impact on jobs.
The
White House claimed in a blog post Jan. 7
that the law "could create more than 300,000
additional jobs" by "slowing the growth of
health care costs." The liberal Center for
American Progress said in
a January 2010 report that "health care
reform could increase the number of jobs in the
United States by about 250,000 to 400,000 per
year over the coming decade." But it remains to
be seen whether the law will actually slow the
growth of costs for employers and individuals,
as the White House hopes it does.
Budget-Busting?
So what about the "budget-busting"
label that House Republicans are also trying to
apply?
The Congressional Budget Office
officially scored the new law as self-financing,
projecting that it would actually reduce
the deficit over the first 10 years and
beyond. And so it should surprise nobody
that
CBO
said Jan. 6 that repealing the new law, as
Republicans propose, would increase the deficit.
CBOs latest figures project that repealing the
new law will increase the deficit by a total of
$230 billion over the next 10 years (through
fiscal year 2021). So keeping it in place would
help the budget, not bust it.
Republicans have a point, to this
extent: The CBO is forced by law to rely on
assumptions that may not turn out to be true,
and which Medicare officials say probably wont
happen. The Medicare systems chief actuary,
Richard Foster,
issued a report soon after passage of the
law saying much of the projected savings "may be
unrealistic," and that the law could cause 15
percent of hospitals to become unprofitable
unless Congress eases up. "If these reductions
were to prove unworkable within the 10-year
period 2010-2019 (as appears probable for
significant numbers of hospitals, skilled
nursing facilities, and home health agencies),
then the actual Medicare savings from these
provisions would be less," Foster said.
If that happens, the law could well
turn out to increase the deficit rather than
trim it. But that remains to be seen.
Sources
Congressional Budget Office. "The
Budget and Economic Outlook: An Update."
Aug 2010.
Republican House leadership. "Obamacare:
A Budget-Busting, Job-Killing Health Care Law."
6 Jan 2011.
Chow, Michael J. and Bruce D.
Phillips. "Small
Business Effects of a National Employer
Healthcare Mandate." NFIB Research
Foundation. 26 Jan 2009.
Sheils, John, senior vice
president, The Lewin Group. Interview with
FactCheck.org. 7 Jan 2011.
U.S. House.
H.R. 2. Introduced 5 Jan 2011.
Congressional Budget Office. "Effects
of Changes to the Health Insurance System on
Labor Markets." 14 Jul 2009.
Novak, Viveca and Lori Robertson. "Health
Care and the Economy." FactCheck.org. 17 Nov
2009.
"Small
Business Looks to the New Congress to Repeal the
Healthcare Law." NFIB website, accessed 7
Jan 2011.
Cutter, Stephanie. "Repealing
the Affordable Care Act will Hurt the Economy."
WhiteHouse.gov. 7 Jan 2011.
House of Representatives Committee
on the Budget, GOP staff. "The
Budgetary Consequences of the Presidents Health
Care Overhaul." accessed 7 Jan 2011.
Congressional Budget Office. "Preliminary
Analysis of H.R. 2, the Repealing the
Job-Killing Health Care Law Act." 6 Jan
2011.
Foster, Richard. "Estimated
Financial Effects of the Patient Protection and
Affordable Care Act, as Amended." Centers
for Medicare and Medicaid Services. 22 Apr 2010.
back to
top
Repeal
of PPACA is the REAL Job-Busting Action
A Republican plan to
sharply cut federal spending this year
would destroy 700,000 jobs through 2012,
according to an independent economic
analysis was released on Monday, February
28, 2011
The rep ort, by
Moody's
Analytics chief economist Mark Zandi,
offers fresh ammunition to Democrats seeking
block the Republican plan, which would terminate
dozens of programs and slash federal
appropriations by $61 billion over the next
seven months. Zandi, an architect of the
2009 stimulus package who has advised both
political parties, predicts that the GOP package
would reduce economic growth by 0.5 percentage
points this year, and by 0.2 percentage points
in 2012, resulting in 700,000 fewer jobs by the
end of next year. His report comes on the heels of a similar
analysis last week by the investment bank
Goldman Sachs, which predicted that the
Republican spending cuts would cause even
greater damage to the economy, slowing growth by
as much as 2 percentage points in the second and
third quarters of this year. Zandi also
had bad news for liberal Democrats who are
resisting sharp spending cuts: Bringing deficits
down to sustainable levels will require more
than a growing economy. Even if the economy
recovers as expected, he writes, lawmakers will
have to cut about $400 billion a year through
the rest of this decade to narrow the gap
between spending and revenue, and stop adding
significantly to the national debt. ort, by
Moody's
Analytics chief economist Mark Zandi,
offers fresh ammunition to Democrats seeking
block the Republican plan, which would terminate
dozens of programs and slash federal
appropriations by $61 billion over the next
seven months. Zandi, an architect of the
2009 stimulus package who has advised both
political parties, predicts that the GOP package
would reduce economic growth by 0.5 percentage
points this year, and by 0.2 percentage points
in 2012, resulting in 700,000 fewer jobs by the
end of next year. His report comes on the heels of a similar
analysis last week by the investment bank
Goldman Sachs, which predicted that the
Republican spending cuts would cause even
greater damage to the economy, slowing growth by
as much as 2 percentage points in the second and
third quarters of this year. Zandi also
had bad news for liberal Democrats who are
resisting sharp spending cuts: Bringing deficits
down to sustainable levels will require more
than a growing economy. Even if the economy
recovers as expected, he writes, lawmakers will
have to cut about $400 billion a year through
the rest of this decade to narrow the gap
between spending and revenue, and stop adding
significantly to the national debt.
"Significant
government spending restraint is vital, but
given the still halting economic recovery, it
would be counterproductive for that restraint to
begin until the economy is creating enough jobs
to bring down the still very high unemployment
rate," Zandi writes.
"Shutting the
government down for any length of time would
also be taking a big chance with the recovery,
not only because of the disruption to government
services, but also due to the potential hit to
the fragile collective psyche."
A partisan brawl is also brewing over the
legal limit on government borrowing, currently
set at $14.3 trillion. In his new report, Zandi
predicts that the U.S. Treasury will be able to
manage the government's finances under that cap
only until June. With Republicans lining up
against an increase, Zandi writes that the
"threat of a serious
policy misstep in the next several weeks and
months" is serious.
back to
top
The Biggest and
Baddest Lies about PPACA ("Obamacare")
I
have been working on a compilation of the
many lies and distortions about PPACA that
have, in many cases become viral on the
Internet. And while most of them are, to the
rational mind at least blatantly and
bold-facedly outright lies, their
repetition, particularly by the likes of
Glenn Beck, Rush Limbaugh, Sean Hannity and
Bill OReilly have embedded them as apparent
truths in the collective conscience of the
Tea-Party and those who have fallen for the
lie.
My list is
not-comprehensive¸ and is still a work in
progress. The list will be updated and
expanded, but as of this haze-filled
morning, here it is:
Lie #1
Obamacare will result in the largest
tax hikes in the history of America.
Ordinary taxpayers will see their taxes
skyrocket." The liars who make
this statement go even further, saying:
The top income tax rate will rise from 35
to 39.6 percent.... The lowest rate will
rise from 10 to 15 percent. All the rates in
between will also rise. Itemized deductions
and personal exemptions will again phase
out, which has the same mathematical effect
as higher marginal tax rates. The liars
base their conclusion on the scheduled
expiration in 2011 of the 2001 and 2003
Bush tax cuts which a then
Republican-controlled Congress established
as a means of getting around Congressional
rules on reporting the actual costs of any
new legislation. By having the tax cuts
expire within 10 years they did not have
to account for the deficits these cuts
created in the federal budget. The liars
assume that Democrats will simply allow
ALL the tax cuts to expire. The fact is that
Democrats have repeatedly said that they
want only the top end tax cuts, those on
individuals earning more than $200,000 a
year and couples earning more than $250,000,
to expire. The tax cuts on lower incomes
will be extended and made permanent. So,
unless ordinary Americans is defined to
include those earning in excess of $200,000
a year, the statement is a lie.
Lie #2
Obamacare has a second "wave" of tax
increases taking effect January 1, 2011 that
impact ordinary Americans. But
this "wave" consists of three relatively
minor tax changes that affect relatively few
people.
·
The so-called
"Obama Medicine Cabinet Tax" simply aligns
rules governing health savings accounts
(HSAs), Flexible Spending Arrangements
(FSAs) and Health Reimbursement Arrangements
(HRAs) with the tax rules that apply to
deducting medical expenses generally. Under
current law, taxpayers in general are not
allowed to deduct the cost of
non-prescription drugs as a medical expense.
The only exception is for insulin. But those
with
HSAs, FSAs and HRAs were allowed to
use pre-tax dollars to buy aspirin,
over-the-counter cold and allergy
medications, and other drugs available
without a doctors prescription. The new
"tax" simply says HSAs, FSAs and HRAs cant
be used to buy these medications -- except
for insulin -- after December 31. This will
affect a small proportion of taxpayers. For
example, the health insurance industry says
10 million persons were covered by HSAs as
of January of this year, roughly 3.2 percent
of the population. For that relatively small
group, the change does amount to a tax
increase. It will bring in a total of $5
billion over the next 10 years.
·
The "HSA
withdrawal tax hike" refers to a doubling of
the current 10% penalty that must be paid on
any HSA funds spent for something thats not
a qualified medical
expenditure. This is expected to
bring in $1.4 billion over 10 years.
·
The "special
needs kids tax" refers to a cap of $2,500
that the new law places on spending from
FSAs. The argument made is that "many"
families with special needs children now use
FSAs to pay tuition at private schools
catering to special needs children, schools
that Obamas opponents say "can easily
exceed $14,000 per year." Perhaps so.
IRS rules do allow use of FSA funds to pay
for such expenses with pre-tax dollars. But
the liars who make this statement offer no
evidence of how many families might be
taking advantage of this tax break
currently. Indeed most employers offering
FSA plans already limit the amount that can
be set aside tax-free, to $2,500-$4,000. The
claim is copied from the website of
Americans for Tax Reform, but as ATR itself
says: "For most people, the $2500 cap
wont be noticed." As ATR concedes, FSAs
"tend to be used for things like small
deductibles, co-payments, eyeglasses,
over-the-counter medicines, and laser eye
surgery." The amount deferred in the
typical FSA is probably much less than
$2,500 today, ATR says. The Congressional
Budget Office expects the change will bring
in $13 billion over 10 years, but says
nothing about how much of that is likely to
come from the pockets of parents of special
needs children.
Without
arguing for or against any of these three
tax increases. I simply point out that, even
taken together, they amount to less than $2
billion per year and, therefore, dont
constitute anything close to a "wave" of
historically large tax increases taking
effect next year.
Lie #3
Obamacare provides for armed IRS
agents to enforce penalties. This is a
fantasy. Tea-Party lawmakers are claiming
the law might require as many as 16,500
new jobs in the IRS, a figure inflated by
dubious assumptions. But the agencys role
will be mainly to hand out tax credits, not
to enforce penalties. And the IRS wont be
sending armed agents to enforce the health
care mandate, as falsely claimed by Texas
Tea-Party Congresscritter Ron Paul. The law
specifically waives any criminal penalties
for those who both decline to obtain
insurance coverage and refuse to pay the tax
enacted to penalize lack of coverage.
Lie #4
Failure to purchase insurance will
result in jail time for
offenders. This is another
bold-faced lie perpetuated over and over
again by the laws opponents, and especially
prevalent among Fox News commentators and
guests. The Facts: The law has a
specific provision: "In the case of any
failure by a taxpayer to timely pay any
penalty imposed by this section, such
taxpayer shall not be subject to any
criminal prosecution or penalty with respect
to such failure,"
which prohibits criminal prosecutions (and
any possible jail time. Fox News
reluctantly and belatedly admitted this
truth. But Fox News Bill OReilly, trying
to defend himself and his network from this
allegation, went so far as to suggest that
no one on Fox News had ever suggested that
there would be jail time. That statement
was debunked by numerous news agencies
citing more than 40 instances when Fox News
commentators and guests lied about jail
time, with at least 3 of these coming from
Bill OReilly himself. See, for example:
http://www.politifact.com/truth-o-meter/statements/2010/apr/27/bill-oreilly/oreilly-says-no-one-fox-raised-issue-jail-time-not/
Lie #5
The law set up a "private army" for
Obama. The facts: The liars who make
this statement refer to a provision in the
new law that establishes a Ready Reserve
Corps of doctors and other health care
workers who can be called upon in the case
of a public health emergency. E-mails that
call them "Hitler youth" and speculate that
they may be administering "lethal
injections" are thoroughly false and
malicious.
Lie #6
-- A government committee will decide
what treatments you will receive."
The facts: The liars who make this statement
refer to a provision in the new law that
establishes a "private-public advisory
committee" that will "recommend" what
minimum benefits would have to be
included in the basic insurance
package that would meet the programs
mandate for coverage. There is nothing in
the law that limits an individual from
coverage of more extensive benefits nor is
there a government panel which will review
each individuals treatments.
Lie #7
-- "Non-US citizens, illegal or not, will
be provided with free healthcare services."
The facts: The liars who make this statement
refer to a provision in the new law that
prohibits discrimination in health care
based on "personal characteristics." Another
provision explicitly forbids "federal
payment for undocumented aliens" and further
prohibits undocumented individuals from even
using their own money to pay for coverage
through the insurance exchanges that will be
created by the new law.
Lie #8
-- Muslim Americans are exempt from the
mandate to have health insurance.
The law does say that some religious groups
may be considered exempt from the
requirement to have health insurance, and it
uses the definition from 26 U.S. Code
section 1402(g)(1), which defines the
religious groups considered exempt from
Social Security payroll taxes. Eligible
sects must forbid any payout in the event of
death, disability, old age or retirement,
including Social Security and Medicare. They
must also be approved by the Commissioner
for Social Security. The law was originally
designed to apply to the Old Order Amish,
and we have yet to find any cases in which
members of other religious groups were
successfully able to claim exemption.
The Muslim faith does not forbid purchasing
health insurance, and no Muslim group has
ever been considered exempt under the
definitions used in the health care law.
Lie #9
Under the new health care law, the
elderly will be denied care when they have
passed the age limit for treatment.
The liars who make this statement are unable
to cite any provision, any reference, or any
speech, comment or off-the-record remark
from any of the bills sponsors or
supporters that justifies this conclusion.
Where can we start, there is absolutely
nothing in the new law, not a sentence, not
an inference, not a scintilla of evidence
that age would be a standard for care or
could become a standard of care. Some lies
are more bold-faced than others. This is one
of them.
Lie #10
A section about Community-based Home
Medical Services is actually a payoff to
ACORN for its support of Obama."
The liars making this statement interpret
any reference to the word "community" to be
some kind of payoff for ACORN, a
community-organizing group long vilified
by President Obamas opponents. ACORN does
not provide medical services, home or
otherwise, and there is no connection,
tangentially or otherwise. In truth,
community-based home medical services and
the development of community-based health
centers have been old pre-Tea Party
takeover Republican proposals as an
alternative to the more direct government
provision of care. Three times in the eight
years of President George W. Bush State of
the Union speeches, Bush called for
Congressional action on expanding
community-based health centers. This just
another good old pre-Tea Party takeover
Republican idea, incorporated into the new
law in an attempt to gain
bipartisan-support, that has been turned on
its head and is now evidence of Obamas
socialism.
Lie #11 Every person
will be issued a National ID Healthcard.
The liars who make this claim refer to a
provision that government standards for
electronic medical transactions "may
include utilization of a machine-readable
health plan beneficiary identification
card, to show eligibility for services.
Insurance companies typically issue such
cards already, but if such a standard were
issued the cards would need to be in a
standard form readable by computers. The
word may is used to permit such a
standard, but it does not require one. There
is no mention of any National ID
Healthcard anywhere in the bill.
Lie #12
-- "The Obama Health and Human Services
Department is planning to compile a federal
health record on all U.S. citizens by 2014,"
including "each individuals Body Mass Index."
The Facts: The liars who make this claim
refer to a provision in the new law that
directs the establishment of an electronic
health record (EHR) by 2014. Other liars
about the bill have cited this same
provision for all sorts of potentially
malevolent and nefarious actions by
government. Lets set the record
straight: the broader use of electronic
health information technology (HIT) has
been a goal of both the private health care
industry, which formed a trade group the
Association for Electronic Health Care
Transactions (AFEHCT) in 1993 and the
government, which established the
quasi-government-private sector Workgroup
on Electronic Data Interchange (WEDi)
in 1991. This was the original brainchild of
Missouri pre-Tea Party takeover Republican
Senator Christopher Bond in 1989 and was a
major part of the Health Insurance
Portability and Accountability Act of 1996
(HIPAA). Some estimates say that better use
of HIT could result in savings of up to 30%
of the health care dollar. Computerizing
medical records has long been a goal of
policymakers across the ideological
spectrum. The idea is to shift from
paper-based records to electronic ones, so
that doctors can access information about
patients more quickly and easily and make
better clinical decisions as a result.
Supporters hope that electronic medical
records will reduce the frequency of medical
errors, unnecessary diagnostic tests and
inappropriate treatments. They also hope
that, in the long term, streamlining
record-keeping could bring down the rapidly
escalating cost of health care. As
noted, the effort did not begin with
President Barack Obama. At the
earliest President George H.W. Bush called
for more work in this area in 1991. In 2004,
his son, President George W. Bush issued an
executive order creating incentives for the
adoption of information technology by 2014,
to be spearheaded by a new federal official,
the national coordinator for Health
Information Technology. Under Obama,
Congress passed his economic stimulus
package in February 2009. The stimulus
included several items designed to promote
health information technology, including $19
billion over four years to fund electronic
infrastructure improvements and the
widespread adoption of electronic health
records by providers, typically through
higher Medicare and Medicaid reimbursements
for doctors who use electronic medical
records effectively. The Office of the
National Coordinator for Health Information
Technology describes the Nationwide Health
Information Network as a "network of
networks." Please note this is not a single
database residing at, say, a federal agency.
It's more accurately viewed as a network to
link many separate databases where records
already exist, such as regional databases or
medical offices, along with efforts to
establish common technical standards so that
these far-flung repositories of data can
exchange information as needed. So will an
intrusive government will have access to
your private medical information? The short
answer is: No. This is just another great
old pre-Tea Party takeover Republican idea
that has gone bad because it was embraced by
Democrats and President Obama. Just say NO
to anything President Obama says.
Lie #13 -- The
federal government will have direct,
real-time access to all individual bank
accounts for electronic funds transfer.
The Facts: The liars who make this claim
refer to a provision that aims to simplify
electronic payments for health services, the
same sort of electronic payments that
already are common for such things as
utility bills or mortgage payments. The bill
calls for the secretary of Health and Human
Services to set standards for electronic
administrative transactions that would
"enable electronic funds transfers, in order
to allow automated reconciliation with the
related health care payment and remittance
advice." There is no mention of "individual
bank accounts" nor of any new government
authority over them. Also, the section does
not say that electronic payments from
consumers is required. Also, this section of
the law simply expands on the 1996 Health
Insurance Portability and Accountability Act
(HIPAA) which was originally proposed by
President George H.W. Bush in 1991 and which
was passed by a GOP-controlled Congress in
1996 and expanded by Republicans in 2004 and
2006. Just another good old pre-Tea
Party takeover Republican-idea gone bad
simply because Democrats also support it.
The Republican/Tea-Party NO-machine gone
amok.
Lie #14 Taxpayers
will subsidize all union retiree and
community organizer health plans (read:
SEIU, UAW and ACORN). The liars who
make this claim refer to a provision that
would set up a new federal reinsurance plan
to benefit retirees and spouses covered by
any
employer plan, not just those run by
labor unions or nonprofit groups.
Specifically, it covers retirees and . . .
spouses, surviving spouses and dependents of
such retirees who are covered by
employment-based plans that provide health
benefits. Its open to any group health
benefits plan that . . . is maintained by
one or more employers, former employers or
employee associations, as well as voluntary
employees beneficiary associations .
Furthermore, the aim of the fund is to cut
premiums, co-pays and deductibles for the
retirees. Payment shall not be used to
reduce the costs of an employer. Since this
provision went into effect, thousands of
corporations, including some of the nations
largest employers, have applied for
coverage.
Lie #15 All
private healthcare plans must conform to
government rules to participate in a
Healthcare Exchange. The liars
who make this claim are trying to draw
negative inferences from a provision in the
new law setting up new state and regional
Health Insurance Exchanges through which
individuals and employers may choose from a
variety of private insurance plans, much
like the system that now covers millions of
federal workers. Any private insurance plans
offered through this exchange must meet new
federal standards. For example, such plans
cant deny coverage for preexisting medical
conditions.
Lie #16
All private healthcare plans must
participate in the Health care Exchange
(i.e., total government control of
private plans.) This is yet
another good old pre-Tea Party takeover
Republican idea gone bad because Democrats
stole it. Health Exchanges have long
been operational in two US states, Utah and
Massachusetts. Under the Utah Health
Exchange, operational for over 10 years and
established by a Republican-controlled
legislature and endorsed by Republican
governors and local business owners, most
Utahans get their health coverage through
the Exchange which assures basic standards
and operational mandates. In Massachusetts,
the states Connector was and is an
integral part of the Romneycare plan
mandating coverage for every state
resident. Under the Obama
version, no insurance company is required to
sell plans through an exchange if it doesnt
want to. Any employer may choose to buy
coverage elsewhere. In fact, the vast
majority of employers will still be buying
private plans through the normal
marketplace, because only employers with 100
or fewer employees are even allowed to buy
through an exchange in the first year. It
wont be until 2017, that the exchanges will
be open to all employers.
Lie #17 Members
of Congress have exempted themselves from
coverage under the law. Au contraire,
Contrary to all rumors suggesting that
members of Congress are NOT covered by the
new law, the law specifically requires that
members of Congress MUST buy their coverage
through an Exchange. Quote: "The
only health plans that the Federal
Government may make available to Members of
Congress and congressional staff with
respect to their service as a Member of
Congress or congressional staff shall be
health plans that are (I) created under
this Act (or an amendment made by this Act);
or (II) offered through an Exchange
established under this Act (or an amendment
made by this Act)."
Lie #18
The new law cover Viagra for convicted
sex offenders. The facts: Theres no
change from current law. Convicts who are
not in prison can purchase whatever health
plan theyd like and some plans could cover
erectile-dysfunction drugs. The
Congressional Research Service said that
there was nothing in the new law that would
"require health plans to limit the type of
benefits that can be offered based on the
plan beneficiarys prior criminal
convictions." This mini-controversy erupted
when Republicans introduced a string of
amendments in a final effort to obstruct
passage of the reconciliation bill.
Republican Sen. Coburn of Oklahoma proposed
the amendment to bar sex offenders from
getting health plans that covered such drugs
with federal money through the state-based
exchanges. Democratic Sen. Max Baucus of
Montana called the amendment "a crass
political stunt." And it failed by a 57-42
vote.
AND THE
BIGGEST, BADDEST LIE ABOUT PPACA OF ALL: It
will kill granny (and impose health care
rationing) --
Trust me on
this, Im a lawyer
just like his Democratic
predecessor in the presidency, Bill Clinton,
who was somewhat successful at reaching
across the aisle, President Barack Obama has
not hesitated to steal a good old pre-Tea
Party Republican ideal and turn it to good
(political) use. Republicans (without a
single Democratic vote) passed the Medicare
Modernization Act of 2003. Buried in that
717-page law were provisions for CM2 to
begin the process of determining the
comparative effectiveness of various
health care services. The current health
care plans simply build on that initial
step
but oops, thats where Sarah Palins
death panels
and killing granny became an issue.
The GOP-passed 2003 Medicare Modernization
Act (better known for establishing the Part
D drug program) had lots of buried secrets,
not the least of which was new funding for
AHRQ and a plan to begin several
demonstration projects with a goal of better
identifying:
the appropriate use of
best practice guidelines
by providers and services by beneficiaries
The
reduced scientific uncertainty
in the delivery of care through the
examination of
variations in the utilization
and
*allocation
of services, and outcomes measurement
and research
achieving the
*efficient
allocation of resources
the financial effects on the health care
marketplace of altering the incentives for
care delivery and changing the
*allocation of resources
(*
Trust me on this, Im a lawyer, allocation
of resources = rationing)
The little agency that could. Buried in the
backwater reaches of the U.S. Public Health
Service is the Agency for Healthcare
Research and Quality (AHRQ), charged with
developing the future cookbook of health
care.
CM2 has already embarked on an
effort to define many of the elements of
effective health care, that is what works
and what doesnt, using much of the work
product of AHRQ.
In the future, we will only pay for what
works and not for what doesnt work.
President George W. Bush, September 17, 2006
Lies and the Big Fat Liars that Tell Them
back to
top
The budgetary impact of the new health
care reform law over 10 years and beyond.
Considerable debate has focused on the ACTUAL effects
the recently enacted health reform legislation (PPACA) would have on
the federal budget. TeaParty/Republicans, led by their new majority
leader, Eric Cantor, have been particularly vocal in reinforcing their
demand that the new law be repealed IN ITS ENTIRETY. Democrats have
countered citing the reports from both the nonpartisan Congressional
Budget Office (CBO) and the bipartisan Joint Committee on Taxation
(JCT).
Let's begin by reviewing the
budget estimates done
by CBO and the staff of the Joint Committee on Taxation (JCT):
In combination, the initial legislation and the
subsequent reconciliation act that modified it will generate changes
in direct spending and revenue that will reduce federal deficits by
$143 billion during the 2010-2019 period. The legislation will change the size of the federal
budget by increasing outlays by $411 billion and revenues by $525
billion over the next 10 years (excluding the provisions of the
reconciliation act related to education, which will reduce spending
by about $19 billion over that period). The legislation will
increase the federal budgetary commitment to health care (the sum of
net federal outlays for health programs and tax preferences for
health care) by $390 billion over the next 10 years. The legislation
will reduce federal deficits during the decade beyond the 10-year
budget window relative to those projected under current lawwith a
total effect in a broad range around one-half percent of GDP. But are these assumptions valid? Eric Cantor of the
TeaParty/GOP says: "About the budget
implications, I think most people understand that the CBO did the job
it was
asked to do by the then-Democrat majority, and it was really comparing
apples to oranges. It talked about 10 years' worth of tax hikes and
six years' worth of benefits. Everyone knows beyond the 10-year
window, this bill has the potential to bankrupt this federal
government as well as the states."
We can conclude then, if Congresscritter Cantor is correct, that the
CBO is not the non-partisan body we have been led to believe
and is simply another partisan hack group, which we should be free to
ignore any time its conclusions threaten our pre-conceived notions.
Aw shucks, before we go that far, let's look at some
of Mr. Cantor's objections:
He has asserted that CBO and JCT have misestimated
("misunderestimated?) the effects of the changes in law,
particularly underestimating the costs of the program subsidies to
low and middle income families.
But, if you look at the tables and the statistics
relied upon by the CBO and JCT, you can see that they have chosen some
fairly expansive numbers, reflecting the middle of the distribution of
possible outcomes based on some pretty careful analysis and using
clearly professional judgment, drawing upon relevant research by other
experts. Of course, their estimates are just that, "estimates," and
the effects of comprehensive health care reforms at this early stage
are clearly very uncertain. Actual outcomes will surely differ from
the CBO and JCT estimates in one direction or another, but to insist
that the TeaParty/GOP estimates are the only ones that are correct and
that the other side's are a crock of you know what, is disingenuous at
best. (For the record, we should note that Democrats have criticized
the CBO estimates as being "too low" and "not fairly estimating the
larger impact the new law will have on budgetary savings). Looking at
the CBO and JCT estimates seems the safest middle ground.
Cantor
and the TeaParty/GOP have also asserted that the CBO and JCT budget
estimates hide or misrepresent certain effects of the law, such as
its impact on future discretionary spending, its effect on the
governments ability to pay Medicare benefits, and its effects on
the economy, suggesting that these impact will be far greater that
suggested.
The CBO and JCT estimates focus on direct spending and revenues
because those are the figures that are relevant to the "pay-as-you-go
rules" that govern House spending legislation. PAYGO is the acronym
for House budget rules first adopted during the Newt Gingrich/GOP
years (post 1994) which were essentially abandoned during the George
W. Bush "borrow and spend" years and restored in 2006 when the
Democrats regained control of the House by a narrow 6-vote margin.
PAYGO rules require that any new spending be offset either by new
taxes or by cuts in spending elsewhere. To go around PAYGO, the House
would have had to pass additional legislation excepting the spending.
In the case of PPACA, the new taxes and spending offsets were
considered neutral and thus additional legislation was not required.
The additional spending suggested by Cantor and the TeaParty/GOP, that
the costs of implementing the new law, and the costs of maintain
physician reimbursement at non-BBA levels, should have invoked PAYGO
and thus demand repeal of the law, fall flat. (1) Administrative
costs have never been considered under PAYGO and were routinely
exempted during years of Republican control of the House, and (2) the
costs of maintaining physician Medicare reimbursement at higher than
the rates under the 1997 Balanced Budget Act, are NOT the costs of
PPACA. They are costs of a separate piece of legislation and, if a
problem for the TeaParty/GOP, they need to be addressed separately. As
the CBO said, those effects will occur without any additional
legislative action and regardless of PPACA.
o
Additionally, the
legislation will improve the cash flow in the Hospital Insurance trust
fund (that is, Part A of Medicare) by more than $400 billion over 10
years. Higher balances in the fund will give the government the legal
authority to pay Medicare benefits longer.
Cantor and his TeaParty/GOP cohorts argue that CBO and JCT 10-year
estimates of total federal budget reduction are flat out wrong
and have asserted that the law will be changed in the future in ways
that will make deficits worse. In fact, CBOs cost
estimate noted that the legislation maintains and puts into effect a
number of policies that might be difficult to sustain over a long
period of time. For example, the legislation reduces the growth rate
of Medicare spending (per beneficiary, adjusting for overall
inflation) from about 4 percent per year for the past two decades to
about 2 percent per year for the next two decades. It is unclear
whether such a reduction can be achieved, and, if so, whether it would
be through greater efficiencies in the delivery of health care or
through reductions in access to care or the quality of care. The
legislation also indexes exchange subsidies at a lower rate after
2018, and it establishes a tax on insurance plans with relatively high
premiums in 2018 and (beginning in 2020) indexes the tax thresholds to
general inflation.
[As another historical
note, one need only look at the passage of Medicare in 1965. Lyndon
Johnson gave away the farm in order to get that law passed in the
first place. Cost-plus reimbursement to hospitals, "usual and
customary" payments to physicians and other providers. Opponents then
made many of the same arguments they are making today; "costs
estimates were too low, it would bankrupt the country, benefits are
not being paid for, we can't afford it." Face facts, the 2010
version of PPACA will not be the 2010 version just as the 1965 version
of Medicare was not the 1975 version (P.L. 92-603 was passed in 1972
changing much of the law), or the 1985 version (DRGs had replaced
cost+ and RB-RVS replaced usual and customary), or the 2011 version.
Amendments will be enacted, circumstances will demand changes, our
laws are living instruments that adapt, modify and reflect as the
nation changes.]
That's
all well and good -- but it's not true. Take Cantor's TeaParty/GOP
core point: The health-care reform bill includes
"10 years' worth of tax hikes and six years' worth of benefits."
There's nothing philosophical about this statement. It can be checked
with a simple look at the spending tables the Congressional Budget
Office published in their analysis of the bill. And when you look at
those tables,
Cantor's statement falls apart:
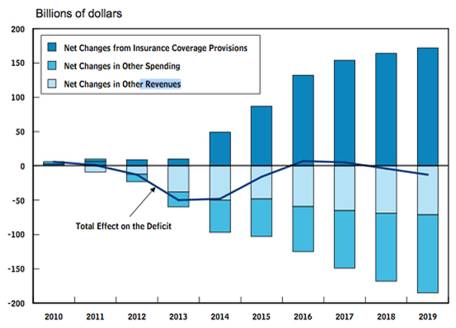
Roughly speaking, new
spending is what counts as "benefits." Those are the lines shooting
up. New taxes are the lighter blue part of bars pointing down. In
years one, two, and three, new benefits are larger than or matched
with new taxes. In year four, that's not true, but the difference is
fairly small. And in the six years after that, even Cantor admits the
benefits match or overwhelm the taxes.
Comparing 10 years of saving and working with six years of spending is
not comparing apples to oranges. Parents will routinely work harder
(revenue increases) and save more (spending cuts) for decades in order
to help their children pay for college. That's 18 years of raising
revenues and cutting costs in return for four years of spending on
benefits. An accountant wouldn't look at that and say he couldn't
assess the wisdom of the decision because it's apples-to-oranges. An
accountant would happily note that that's how you pay for things when
you're being responsible. Cantor's party might be out of practice on
that, given the way they paid -- or, to be more specific, didn't pay
-- for the Medicare Prescription Drug Benefit, but it doesn't make it
any less true.
As for the period "beyond the 10-year window," the Congressional
Budget Office -- which is now comparing "apples to apples," as the law
is delivering full benefits for all 10 of the next 10 years -- says
the law saves vastly more money in its second decade: "The legislation
will reduce federal deficits during the decade beyond the 10-year
budget window relative to those projected under current lawwith a
total effect in a broad range around one-half percent of GDP." That's
in the neighborhood of
a trillion dollars.
What's important about Cantor's argument is not that he's wrong. It's
why he's saying something he knows to be wrong. There are
plenty of reasons to oppose the health-care reform bill. You might not
want to spend that money insuring people, or you might not think the
legislation goes far enough in reforming the system. But as a matter
of arithmetic, using the math that Congress always uses, the bill
saves money. It cuts enough spending and raises enough taxes to more
than pay for itself, both in the first 10 years and in the second 10
years. In fact, Democrats added that second metric, which is not
typically a hoop that legislation has to jump through, in order to
specifically allay concerns that the legislation would backload its
costs. Instead, as CBO said, it ramps up its savings.
But Cantor and the TeaParty/GOP know full well that the bill is
unpopular largely because people think it increases the deficit. Polls
have
shown
that only 15 percent of Americans know that CBO said it will reduce
the deficit. If, in the repeal fight, it becomes widely understood
that the bill reduces the deficit, it will become more popular. So
it's crucial, as the repeal effort goes forward, for
TeaParty/Republicans to become much more brazen in falsely asserting
that the bill doesn't really reduce the deficit, and that even if the
CBO does say it reduces the deficit, that they're saying that because
they've been tricked somehow. But CBO wasn't tricked. If it were,
Cantor, who has a staff dedicated to figuring these things out, would
have a better argument than the one he's offering.

Everything You Ever Wanted to Know About the
PPACA Independent Payment Advisory Board But
Were Afraid to Ask
The Patient Protection and Affordable Care
Act established a 15-member IPAB to extend
Medicare solvency and reduce spending growth
through the use of a spending target system
and fast-track legislative approval process.
By April 30 of each yearbeginning in
2013the Centers for Medicare & Medicaid
Services (CMS) Actuary's Office will project
whether Medicare's per-capita spending
growth rate in the following two years will
exceed a targeted rate. Initially, the
targeted rate of spending growth will be
based on the projected five-year average
percentage increase in the Consumer Price
Index for all urban consumers and the
Consumer Price Index for all urban consumers
for medical care.
Beginning in 2019, the target will be set at the nominal gross
domestic product per capita + 1.0 percent.
If future Medicare spending is expected to
exceed the targets, the IPAB will propose
recommendations to Congress and the
president to reduce the growth rate. The
IPAB's first set of recommendations would be
proposed on Jan. 15, 2014.
Spending rate reductions will be established
at:
0.5 percent in 2015
1.0 percent in 2016
1.25 percent in 2017
1.5 percent in 2018 and beyond
If Congress fails to pass legislation by
Aug. 15 each year to achieve the required
savings through other policy changes, the
IPAB's recommendations will automatically
take effect. The IPAB is prohibited from
submitting proposals that would ration care,
increase revenues, change benefits, modify
eligibility, increase Medicare beneficiary
cost-sharing (including Parts A and B
premiums), or change the beneficiary premium
percentage or low-income subsidies under
Part D. Hospitals and hospice will not be
subject to cost reductions proposed by the
IPAB from 2015 through 2019. Clinical labs
would be exempt for one year.
Beginning July 1, 2014, the IPAB must also
submit an annual report providing
information on system-wide health care
costs, patient access to care, utilization
and quality of care that allows comparison
by region, types of services, types of
providers, and payersboth private insurers
and Medicare. By Jan. 1, 2015, and at least
every other year thereafter, the IPAB will
submit recommendations to slow the growth in
national health care expenditures while
preserving or enhancing quality of care.
These recommendations could be those that:
(1) the secretary of Health and Human
Services (HHS) and other federal agencies
could implement administratively; (2) may
require federal legislation to be
implemented; (3) may require state or local
government legislation to be implemented; or
(4) private entities can voluntarily
implement.
Fast-track
Legislative Process
By Jan. 15 of each year, beginning in 2014,
the IPAB must submit a proposal to Congress
and the president for achieving Medicare
savings targets in the following year.
If the IPAB fails to submit a proposal to
Congress and the president by Jan. 15, the
HHS secretary must submit a proposal for
meeting the savings targets to the president
and the Medicare Payment Advisory Commission
(MedPAC) by Jan. 25 of that same year. The
president must submit the secretary's
proposal to Congress within two days.
The House and Senate Majority Leader or
their designee must introduce the IPAB
proposal the same day it is received (or on
the first day the chamber is in session). If
the proposal is not introduced within five
days, any senator or representative can
introduce it.
The proposal must be referred to the Senate
Finance Committee and the House Ways and
Means and House Energy and Commerce
Committees.
By April 1, the committees of jurisdiction
are to complete their consideration of the
proposal. Any committee that fails to meet
that deadline will be discharged from
further consideration.
Congress cannot consider any bill or
amendment that does not meet the IPAB
targets or that would repeal or change the
fast-track congressional consideration
process without a three-fifths vote (60) in
the Senate. Non-germane amendments are not
permitted.
The HHS secretary must implement the IPAB
proposal on Aug. 15 of the year in which the
proposal is submitted. Recommendations
regarding the physician fee schedule would
take effect on Jan. 1 the following year. If
Congress does not pass the proposal before
Aug. 15, or if the president vetoes the
proposal as passed by Congress, the original
IPAB recommendations would take effect. (All
policy changes affecting physicians that are
not part of the physician fee schedule will
be addressed in the regulatory process and
will take effect as soon as practicable.)
IPAB Board
Members
The IPAB members are to include:
Fifteen members appointed by the president,
by and with the advice and consent of the
Senate; in selecting individuals for
nominations for appointments to the board,
the president shall consult with: (i) the
majority leader of the Senate concerning the
appointment of three members; (ii) the
speaker of the House of Representatives
concerning the appointment of three members;
(iii) the minority leader of the Senate
concerning the appointment of three members;
and (iv) the minority leader of the House of
Representatives concerning the appointment
of three members
The HHS secretary, the administrator of CMS,
and the administrator of the Health
Resources and Services Administration (all
of whom will serve ex officio as nonvoting
members of the Board)
Qualifications/requirements for IPAB
members:
Appointed members of the IPAB will include
individuals with national recognition for
their expertise in health finance and
economics, actuarial science, health
facility management, health plans and
integrated delivery systems, health
facilities reimbursement, allopathic and
osteopathic physicians, other providers of
health services, and other related fields
who provide a mix of professionals, broad
geographic representation, and balance
between urban and rural areas.
IPAB members must include (but not be
limited to) physicians and other health
professionals, experts in the area of
pharmaco-economics or prescription drug
benefit programs, employers, third-party
payers, individuals skilled in the conduct
and interpretation of biomedical, health
services, and health economics research, and
expertise in outcomes and effectiveness
research and technology assessment. Members
must also include individuals representing
consumers and the elderly.
Individuals who are directly involved in
providing or managing the delivery of
Medicare items and services may not
constitute a majority of IPAB's membership.
The president must establish a system for
public disclosure by IPAB members of any
financial and other potential conflicts of
interest.
No IPAB member may be engaged in any other
business, vocation or employment
back
to top
Let's Just Allow the
Buying of Health Insurance Across State Lines,
That's the Ticket, Cheaper Insurance... NOT!
Another Failed TeaParty/GOP Idea
Recent TeaParty/GOP proposals about buying
health insurance across state lines have sent
many of us scrambling to check policies, and
wondering whether such changes might mean its
time to find a new insurer. After all,
wouldnt such a change open up the market and
make it possible to get cheaper coverage?
Unfortunately, its by no means certain
that such a change would be largely
beneficial. In fact, its actually possible
that the end result might be more expensive
insurance overall, and that over time, more
Americans would find health insurance too
expensive.
So what does selling coverage across state
lines actually mean? Simply that an insurer
could sell their product to any person in any
state. Theoretically, this would mean
consumers have a much greater range of
insurers from which to choose, meaning
increased competition and lower premium costs.
However, there are some wider implications.
The fact is, such a change may end up
benefiting only those who are young, fit, and
healthy people who are low-risk in the eyes
of insurers, and who can have their pick of
policies. Anyone who is moderate or high risk
will eventually find that getting affordable
insurance, or perhaps even any insurance at
all, becomes much harder.
This may seem counter-intuitive. After all,
surely opening up the market will mean
everyone has a better shot at getting
affordable insurance. The problem is, however,
to an insurance company risk is still risk.
The perceived risk of an individual who is
fifty years old, overweight, and a smoker
wont decrease just because that individual
can buy insurance anywhere in the country.
And if an insurance company can offer cheap
premiums to entice low-risk people from all
over the country, theyre that much less
likely to continue offering any type of
insurance to higher-risk individuals.
What this means is, its more likely that
insurers will be encouraged to underwrite more
and more aggressively, with cheaper premiums
for those who qualify as low-risk. But those
cheaper policies will provide increasingly
skimpy coverage, meaning that people who
prefer more comprehensive policies as well
as high-risk individuals will find fewer
companies are willing to offer the insurance
they need.
Does this mean across-state-lines insurance
cant work? Not necessarily, but more thought
is needed to produce a workable solution.
Federal regulation of insurance companies
might be a good start and in fact, if
insurance companies are allowed to sell across
state lines, this might seem to be the most
appropriate and logical solution.
http://www.ftc.gov/bcp/edu/microsites/medicaldiscountscams/index.shtm
Insurance Across State Lines:
Sounds Good... on Paper ... But Consider
the Real Impact ... And Besides it Does
NOTHING to Solve Insurance Affordability and
at Best Might Get Another 4 Million Insured...
A Drop in the Bucket
The Kaiser Family
Foundation has issued a white paper
(reproduced below) on the issue of buying
health insurance across state lines, a key
element in the new GOP Pledge To America,
the Republican plan to unravel much of the
Obama administrations policies, especially the
new Patient Protection and Affordable Care Act
(PPACA). I have interposed a few just
between you and me comments on the Kaiser
white paper.
According to Kaiser:
When Republican House leaders recently
unveiled their 'Pledge
To America,' they revived an idea long
popular with conservatives: legislation that
would allow consumers to buy health insurance
across state lines so that residents of a
state with expensive health plans could find
cheaper options elsewhere.
Just between you and me
cool
idea if it werent for all the fraud artists
and fly-by-night operators out there who are
already preying on the uninsured, people with
pre-existing conditions and more critically
the UNDERINSURED. Weak state insurance laws
and enforcement would open a floodgate for
abuse. More on this later
Advocates of the
Republican proposal -- including some insurers
and small business groups -- say it would give
the more than 17 million Americans who buy
individual coverage a greater choice of plans
and the possibility of lower prices.
When they were writing the new health law,
Democrats said they heard the GOP and they
included a way to sell insurance across state
boundaries. They put in language allowing
states to establish "health care choice
compacts." But Republicans say that the
compacts won't bring the same benefits.
Just between you and me
They
dont explain why or how this would happen,
they simply assert the allegation unsupported
Consumer advocacy groups
are part of the political back-and-forth,
arguing that such provisions would erode many
state protections, leave policyholders with
inadequate coverage and could actually lead to
higher premiums for some people.
With the issue back in
the news, heres a short primer:
What currently restricts insurers from selling
policies outside of their home states?
Insurers are allowed to sell policies only in
states where they are licensed to do business.
Most insurers obtain licenses in multiple
states. States have different laws regulating
benefits, consumer protections and financial
and solvency requirements. Even before the
federal health law was passed, states could
have opted to set up compacts for health
insurance. But they did not.
What do advocates say are the main advantages
of the Republican plan to allow insurers to
sell across state lines?
The individual health insurance market is
dominated in many states by just a handful of
companies, so this provision would allow
consumers to shop broadly for cheaper
policies, supporters say.
"You shouldn't limit
people to products in the states they live in
or make them move to get the insurance they
want," Tom Miller, a resident fellow at the
American Enterprise Institute said.
J.P. Wieske, the
executive director of the Council for
Affordable Insurance, which represents
companies selling individual health insurance,
said replacing the compacts with a GOP
proposal would simplify operations for
insurers. In addition, it will improve
conditions "in a number of states that have
ruined their market" by rigidly regulating
policies. That has left consumers with higher
rates and less competition, he said.
Just between you and me
Oops, there they go again. Regulation is
always bad, and everyone knows that
de-regulation has worked so well to save money
for everyone
NOT! Tell that to Americans
paying off the costs of de-regulating the
nations banking and financial industries.
Under the Pledge to America, the GOP
apparently wants to do the same for the health
insurance industry that it did for banking and
finance.
The Republican plan is
hoping to help turn those states into more
competitive marketplaces, he added. They
haven't been able to do it on their own.
Why is there skepticism about the Republican
concept?
"It's not the concept that is the problem.
Quite the contrary, it's a fine idea," said
Ron Pollack, founding executive director of
Families USA, a consumer health care advocacy
group. But he expressed concern about efforts
to de-regulate the market. "The real
underlying issue is that Republicans and
others who created this do not want to create
adequate standards for the sale of health
care." That would result in policies that
"perpetuate the practices that have harmed
consumers," he said.
If insurers can sell
beyond state lines, the concern is that
consumers would be attracted to the least
comprehensive policies because they would be
cheapest - some call it "a race to the
bottom." For example, someone could buy a
policy in a state that doesn't mandate
coverage of diabetic supplies and then the
consumer could be stuck with higher bills.
In addition, insurers
selling across state lines might market
policies to younger, healthier individuals.
That could leave the insurance pool with older
and sicker individuals, who would face
ever-rising rates -- or face being turned down
-- because their insurers would have fewer
healthy people to spread risk.
That would "undermine
insurance regulation in states doing serious
regulation," said Linda Blumberg, a senior
fellow at the Urban Institute's Health Policy
Center. "It would be destructive to those
state efforts."
There are also fears that consumers dealing
with out-of-state companies would have
difficulties resolving disputes. And, since
health costs vary geographically, insurance
purchased in one state might not cover as much
of the cost of care in a more expensive state.
The federal health law
backers say that it allows the advantages of
cross-border sales while still protecting
consumers. "I think we're going to see a whole
lot more choice available for consumers under
the new law," said Pollack.
How would the new "state
compacts" work?
The new health law allows
states to form insurance compacts but does not
require that they do. States joining a
compact, however, would be required to pass
legislation authorizing that decision. States
could begin the process starting Jan. 1, 2016.
Many of the details for
the compacts will depend on federal
regulations that have not been written yet,
but plans in the compact must meet the new
federal minimum requirements set in the health
law and would be governed by the laws of the
state in which the policies are "issued or
written."
Setting up a compact
would be complex since states would likely
have to settle a number of questions about
regulation and consumer safeguards, said
Blumberg. Because of those types of
bureaucratic issues and because many of the
concerns about getting adequate health
coverage are alleviated by the new federal
law, she said, "I don't think much of this is
going to happen."
The law also requires
that the Office of Personnel Management, which
oversees health benefits for federal
employees, contract with insurers to offer at
least two multi-state plans. They would be
offered through the health insurance
"exchanges" - marketplaces being set up in
2014 to provide individual and small market
coverage. The multi-state plans would be
priced locally. According to the law, these
plans would have to meet the same requirements
as other plans in the exchanges. States could
add more benefits to the plans, although the
states would have to bear the costs.
Why are Republicans
critical of how Democrats handled the issue?
Conservatives say that the high minimum
standard to which all plans must adhere in the
health law works against consumer choice and
that the GOP's market-based system would allow
growth of innovative plans that meet
consumers' needs.
The Republican
proposal "is a serious, honest concept that is
worth doing, if you don't promise the moon,"
said
AEIs Miller. He acknowledged that any
such effort would need a framework to ensure
consumer protections, solvency standards and
accountability but he believes those measures
would not be as restrictive as the provisions
now in the federal health law.
He says that other
industries that were once strictly
state-based, such as banking, have worked well
with interstate competition. "It doesn't mean
you're not regulated," he said. "You'll have
better competition," and still have
safeguards.
...
"Everyone" knows that Obama's health care plan will end up rationing
health care in American, right? ... NOT!
The
"rationing" argument is perhaps the most insidious lie being spread
about PPACA. PPACA has simply built on a really good, original
Republican idea ... "comparative effectiveness" ... the only problem
is that now that Obama and the Democrats have embraced it, the idea
had to be defeated. A good idea gone bad... for one reason and one
reason only ... politics! ...
The GOP-passed 2003 Medicare Modernization Act
(better known for establishing the Part D
drug program... and passed by a GOP-controlled Congress without a
single Democratic vote, in the dead of night, using an esoteric
parliamentary procedure known as "reconciliation" and signed by a
Republican president)
had lots of buried secrets, not the least of
which was new funding for a little government agency known as the
Agency for Health Review and Quality (AHRQ) and a plan to begin
several demonstration projects with a goal of better identifying
... the appropriate use of
best practice guidelines by providers and
services by beneficiaries
The
reduced scientific uncertainty
in the delivery of care through the examination of variations in the
utilization and *allocation of services, and outcomes measurement
and research
achieving the
*efficient allocation of resources
the financial effects on the health care marketplace of altering
the incentives for care delivery and changing the *allocation of
resources
Trust me on this, I am a lawyer...
"allocation of resources
(efficiently or otherwise) is just a neat
little legalistic comfort word for "rationing" ... in the future
said George W. Bush, "we will only pay for what works not for what
doesn't."
That's right, I said GEORGE W. BUSH!
"In the future, we will only pay for what works and not for what
doesnt work.
President
George W. Bush, September 17, 2006
HIPAA facilitates the
collection of data and thus the ability of planners and payers to
ration health care intelligently.
Future of US Health Care: Rationing
by any other name
AHRQ:
The little agency that could: Buried in the backwater reaches of the
U.S. Public Health Service is the Agency for Healthcare Research and
Quality (AHRQ), charged with developing the future cookbook of
health care.
CM2
has already embarked on an effort to define many of the elements of
effective health care, that is what works and what doesnt, using
much of the work product of AHRQ.
Worthless Lives Under the British NHS
People such as scientist Stephen Hawking wouldn't have a chance in
the U.K., where the National Health Service wo uld
say the life of this brilliant man, because of his physical
handicaps, is essentially worthless. uld
say the life of this brilliant man, because of his physical
handicaps, is essentially worthless.
Investors
Business Daily, August 11, 2009
Apparently, Investors Business Daily doesnt have access to the
Internets... A quick stop at Wikipedia would have told them that
Hawking is British, lives in Britain, and has lived to the age of 67
there, and was diagnosed with ALS under, and treated by the National
Health Service for his entire adult life. They must have just been
fooled by his voice synthesizer's American accent.
"I wouldn't be here today if it were not for the NHS. I have
received a large amount of high-quality treatment without
which I
would not have survived."
Stephen
Hawking, at a press conference after being awarded the USAs highest
civilian award, the Presidential medal of Freedom, August 12, 2009.
How Efficient Allocation of Resources
(i.e., Rationing) Would Actually Work
Collect all-population, all-patient, all-payer data (including care
processes, clinical outcomes, patient experiences, and costs while
enabling benchmarking and monitoring of changes)
Assess health outcomes (e.g., percent diabetes under control; cancer
survival rates)
Post web comparison of insurance choices, costs and benefits,
experiences; include share of premium for
administrative/overhead/profit (complete national transparency with
capacity for state or geographic analysis and benchmarks and
designed so states could add, build with more detailed data where
available)
And someday
actually start paying only for what works and not for
what doesnt
IS COMPARATIVE EFFECTIVENESS SIMPLY
ANOTHER WAY OF SAYING RATIONING?
In the
U.K., the National Heath Service (the nationalized health program)
has instituted a National Institute for Health and Clinical
Excellence (NICE).
NICE
has used cost calculations per "quality adjusted life-year (QALY)"
saved as an index for what NHS will or will not cover. Anything
that costs more than £30,000 British pounds (about $54,000 U.S.) per
QALY saved can only be covered after undergoing a further extensive
cost-benefit analysis.
DOES
A QALY MEASURE THE VALUE OF HUMAN LIFE?
The
quality-adjusted life year (QALY) is a measure of disease burden,
including both the quality and the quantity of life lived. It is
used in assessing the value for money in a medical intervention.
The
QALY is based on the number of years of life that would be added by
the intervention. Each year in perfect health is assigned the value
of 1.0 down to a value of 0.0 for death. If the extra years would
not be lived in full health, e,g., if the patient would lose a limb,
or be blind or have to use a wheelchair, then the extra life-years
are given a value between 0 and 1.

Among the leading U.S. developers of QALYs in health care
decision-making AND PAYMENT approval... private commercial insurance
companies.
back to top
Too Many Doctors? Too Few Nurses!
Jeanne's Note: In 1995, I wrote
an article for the magazine then called
"Computers in Health Care." In it I made one of
my famous (infamous???) prescient (but clearly
delayed) predictions, saying that 20 years in
the future (then 2015) the nation would need
only about 450,000 physicians (presently we have
about 800,00), Almost all of these would
be highly-trained specialists. Most primary
care, routine, preventive, well-baby, normal
pregnancy care would be provided by legion of
very highly trained and educated "physician
extenders." (I still have problems with the
terms "physician assistant" but less so with
"nurse
practitioner" which by their very nature imply
limitations.) These would be I said
well-educated (Masters Degree+), well-trained
(1-2 years internships and residencies),
well-compensated (my suggestion in 1995 dollars
was around $100k/year), professionals. ... And
of course, the article resulted in enormous
amounts of "hate mail" primarily from
physicians.
My vision,
given my Michigan and particularly Detroit auto
industry childhood growing up background was of
"CAD-CAM." CAD-CAM was then the "hot" new things
for the auto industry which was "guaranteed" to
make the Big 3 auto companies more profitable
and more successful in competing with their
German and Japanese competitors (the South
Koreans weren't yet that big of force). CAD-CAM:
"computer assisted design/computer assisted
manufacture" was to save the U.S. auto industry.
Well we all know how well that worked out
<sigh>. My CAD-CAM stood for something
different:
computer-assisted
diagnosis/computer-assisted medicine.
My vision: a million or more of these primary
care providing professionals, meeting America's
primary care needs in inner cities and rural
communities, in suburbs and retirement
communities using automation and computer tools
to assist in providing primary and preventative
care.
A new report released on October
5, 2010 may give nurses with advanced degrees a
potent weapon in their perennial battle to get
the authority to practice without a doctor's
oversight. The Institute of Medicine
report says nurses should take on a larger and
more independent role in providing health care
in America, something many doctors have
repeatedly opposed, citing potential safety
concerns. It calls for states and the federal
government to remove barriers that restrict what
care advanced practice nurses ... those with a
master's degree ... provide and includes many
examples of nurses taking on bigger
responsibilities. "A qualified health care
professional is a terrible thing to waste," Cheryll Jones, a pediatric nurse practitioner in
Ottumwa, Iowa, told the authors. The report
calls for elimination of "regulatory and
institutional obstacles" including limits on
nurses "scope of practice" ... which are state
rules about what care people who are not
physicians can provide.
 The
findings come from the Committee on the Robert
Wood Johnson Foundation Initiative on the Future
of Nursing, a collaboration among nurses,
doctors, health care business leaders and
academics that studied the issue for two years.
While the report addresses a ongoing battle
being played across state legislatures, it's not
clear if the new report will have any impact on
those battles. The panel is planning a meeting
next month to discuss ways to implement its
recommendations. The
findings come from the Committee on the Robert
Wood Johnson Foundation Initiative on the Future
of Nursing, a collaboration among nurses,
doctors, health care business leaders and
academics that studied the issue for two years.
While the report addresses a ongoing battle
being played across state legislatures, it's not
clear if the new report will have any impact on
those battles. The panel is planning a meeting
next month to discuss ways to implement its
recommendations.
The new federal health care law provides more
funding for nursing education and nurse-led
clinics, but this study could also propel the
nurses' argument for more authority to deliver
care independently from physicians.
"We cannot get significant improvements in
the quality of health care or coverage unless
nurses are front and center in the health care
system ... in leadership, in education and
training, and in the design of the new health
care system," said Donna Shalala, a former
Health and Human Services secretary and chair of
the IOM's committee on the future of nursing.
"We can't be fighting with each other if we
really are going to have a high quality system
that we can afford."
For years advanced practice nurses ... as well as
a host of other caregivers such as chiropractors
and physical therapists ... have butted heads with
doctors over "scope of practice" considerations.
Doctors maintain that even with an advanced
degree, these nurses do not have the same
education that physicians get in medical school
and residency programs and that patient safety
could be compromised. They are also wary that
their practices could see significant patient
losses if the nurses were allowed to practice
more independently.
In its recommendations, the committee said
Medicare and Medicaid should reimburse advanced
practice nurses the same as a physician for
providing the same care. "When you do the
same job you ought to be paid the same,"
Shalala said.
Also, the report calls for nurses to be allowed
to admit patients to the hospital or to a
hospice and for the Federal Trade Commission and
the Department of Justice to review existing
scope of practice provisions for
"anticompetitive" practices.
The Obama administration has signaled its
commitment to increasing the number of primary
care providers, including nurses. Late last
month the Department of Health and Human
Services announced $320 million in
grants
to strengthen the health care workforce. The
grants include $31 million to 26 nursing schools
to increase full-time enrollment in primary care
nurse practitioner and nurse midwife programs
and $14.8 million for nurse-managed health
clinics. In addition, Peter Buerhaus, a
registered nurse,
heads
the newly formed National Health Care Workforce
Commission, which was set up under the new law
to advise lawmakers on how to change the health
care workforce to better fit America's needs.
Experts predict that more physicians, nurses and
other medical professionals will be needed to
care for the 32 million additional Americans who
will get coverage beginning in 2014 under the
sweeping health care law. Nurses' groups say
that they can help ease a physician shortage.
Last week, the Association of American Medical
Colleges said in a
report
that in 2015, there will be a shortage of nearly
63,000 doctors across all specialties in
America.
Dr. Rebecca J. Patchin, a former nurse who is
now anesthesiologist and member of the American
Medical Associations Board of Trustees, said
that physicians must be involved to help protect
patients. "We think that care in the
operating room or care in the office is best
done with physician involvement and oversight," Patchin said. "Due to that additional training
that they have
when or if a complication
occurs they are better equipped to handle it."
The battle is being waged across the country.
Colorado, for instance, recently became the 16th
state
to allow
nurse anesthetists to work without a doctor's
oversight. In Michigan, nurses are pushing for
legislators there to allow advanced practice
nurses to prescribe drugs. Other fights over
scope of practice for registered nurses loom in
Kentucky, North Carolina, Iowa and Minnesota.
But, Dr. Alexander Hannenberg, president of the
American Society of Anesthesiologists, said the
clashes between nurses and doctors scare the
public. "It's exactly what people worry about
when they worry about what health reform will
bring," he said. "Patients and voters
say ''f you're talking about taking the docs out
of my health care, I want no part of it.'"
Taming the Unicorn: Accounting for Accountable
Care Organizations...
From California Healthline:
Spotting a Unicorn: ACOs Inch
Closer to Reality
Almost everyone can describe
a unicorn -- but has anyone actually seen one?
 The mythical beast is an apt
analogy for the emerging "accountable care
organization" model, according to a
cautionary note from Mark Smith, president
and CEO of the California HealthCare
Foundation. CHCF publishes California
Healthline. The mythical beast is an apt
analogy for the emerging "accountable care
organization" model, according to a
cautionary note from Mark Smith, president
and CEO of the California HealthCare
Foundation. CHCF publishes California
Healthline.
Health
care providers are rushing to create
new structures that could eventually
qualify as ACOs, putting them in line for
added reimbursements under health reform. But
are these actually ACOs? Federal agencies
haven't finished defining the model, and
regulators have yet to bless these new
alliances.
As a result, there's
another word that could describe some would-be
ACOs: illegal. If providers aren't careful,
their new networks may violate current laws
restricting provider competition. Essentially,
the pace of changes wrought by health reform
has outstripped a 14-year-old
legal framework.
Providers Likely in Clear for Now, but Face
Outstanding Legal Questions
Most providers trying to
set up ACOs are probably in the clear,
Modern Healthcare notes. Hospitals
are generally using existing safe harbors,
like direct physician employment and the
Federal Trade Commission-sanctioned Clinical
Integration model, to craft accountable care
alliances.
The government's open
intention to encourage creative structures, in
hopes of unearthing new cost-cutting
strategies, also could absolve progressive
organizations from prosecution. Jon Leibowitz,
FTC chair,
told the American Medical Association in
June that if providers "join together to
improve patient care and lower costs, not only
will we leave you alone, we'll applaud you."
After all, the ACO model
was at the heart of the health reform goal of
more-coordinated care at lower cost. The
concept isn't new. Encouraging
hospital-physician alliances to coordinate
care builds off years of research, failed
projects by care providers themselves and the
government's own efforts to spark clinical and
financial integration.
What is new is that CMS
is clearly willing to "reimburs[e] integrated
providers for providing a broad base of care
to patients,"
according to John Liethen, a health law
attorney with Dorsey & Whitney.
Through the Shared
Savings Program,
Medicare will reward ACOs for reducing total
cost of care for an assigned population of
patients. This reimbursement concept
will initially be voluntary, but is meant to
eventually encompass the entire Medicare
population. Having providers experiment with
different models serves CMS' purposes.
However, that hasn't
stopped health care stakeholders from
grappling with significant legal concerns. How
will regulators interpret physician payments
given anti-kickback statutes? Will these new
ACOs violate existing anti-trust rules? And
what will ACOs look like in California, given
corporate practice of medicine laws that
prevent hospitals from directly employing
physicians?
Agencies Slowly Move Forward
After months of these
questions, some answers may be on the horizon.
FTC, CMS and the HHS
Office of Inspector General next week will
host an
all-day open workshop designed to foster
conversation and address potential changes to
ease ACO development under current law. The
workshop has drawn dozens of key health care
stakeholders, and many participants already
have filed comments ahead of the session. For
example, the American Hospital Association
submitted questions asking for federal
guidance on anti-trust, Stark and civil
monetary penalty laws.
One reason that federal
guidance has been slow to come is that
regulators "are doing much the same thing as
providers: They are scrambling to understand a
changing landscape as it morphs around them,"
Modern Healthcare reports. Susan
DeSanti, a director at FTC, notes that next
week's session will allow the agencies to
collaboratively prepare for situations where
one regulator -- say, CMS -- might deem a
provider worthy of ACO incentive payments,
while FTC submits an anti-trust complaint to
the same provider.
Meanwhile, numerous trade
groups and pilot projects continue to move the
ACO discussion forward. The California
Association of Physician Groups will convene a
national conference on ACOs in late
October. CMS will release guidelines for its
flagship ACO demonstration in December. Still,
many hospitals and physicians have elected to
wait to form or join an ACO until the model is
better defined or regulators switch course.
Interim Strategies Rely on Safe Harbors
Barring further guidance,
providers that are moving ahead with ACOs
essentially have two options to stay on the
right side of anti-trust law: Turn to
hospital-physician employment or
FTC's Clinical Integration model.
Of course, California
hospitals and health systems -- governed by
strict corporate practice of medicine laws --
can't directly employ physicians. Similarly
restrictive laws may also constrain the
model's potential application in states like
Texas and Illinois.
According to Don Ammon, former CEO of
Adventist Health, "for ACOs to work ...
legislative reform would have to occur" in
California.
However, many of
California's independent physician
associations might meet the financial risk
test that would allow them to joint contract
without violating anti-trust law, as they
exclusively operate under capitation
arrangements, Liethen of Dorsey & Whitney
points out. Beyond anti-trust, California's
unique experience with managed care could give
state providers a leg up on attempting the
model.
More broadly, Liethen
notes that "the path to ACOs runs through the
FTC." Notably, the commission's
sanctioned Clinical Integration model relies
on organizations engaging in active evaluation
and modification of physician practice
patterns and cooperating with them to cut
costs and boost quality. Charles Wright, a
partner with Davis Wright Tremaine,
adds that providers "can exist comfortably
within the existing antitrust laws even
without financial risk sharing, if they are
sufficiently integrated clinically."
Here's a look at what
else is making news in health reform.
Health
Reform Rollout
- Last week, President
Obama convened a meeting with more than two
dozen people in the backyard of a family's
home outside of Washington, D.C., to discuss
the benefits of the federal health reform
law (Stolberg,
New York Times, 9/22).
Obama delivered a brief speech, during which
he highlighted new
health insurance industry regulations
that took effect on Sept. 23. The president
also asked guests to share how they hope to
benefit from the health reform law (Aizenman/Kornblut,
Washington Post, 9/23).
- Last week, the
Government Accountability Office announced
the appointment of 19 members to the board
of the not-for-profit Patient-Centered
Outcomes Research Institute, which was
created under the federal health reform law.
PCORI is designed to research the best
medical treatments for patients. The board
members serve staggered six-year terms and
can be reappointed once (Pecquet, "Healthwatch,"
The Hill, 9/23).
- CMS
officials are not content to wait until
Medicaid eligibility significantly expands
in 2014 and are trying to boost program
enrollment now, according to CMS Director
Cindy Mann. Mann said at a public meeting of
the new Medicaid and CHIP Payment and Access
Commission that the agency is breaking out
of the mindset that there will always be an
"eligible but unenrolled" population for
Medicaid and CHIP. She said the agency's
"new paradigm" suggests that "eligibility
equals enrollment" (Reichard, CQ
HealthBeat, 9/24).
- Fewer residents than
expected have enrolled in the high-risk
health insurance pools created in each state
under the federal health reform law. The
pools are designed to serve people with
pre-existing conditions who have not had
health insurance for at least six months.
Enrollment began in some states on July 1,
but others have just recently begun
accepting applications. Officials say that
some states have had fewer than 100
applicants for their high-risk pools,
despite estimates that hundreds of thousands
of residents could qualify for the programs
(Adams, CQ HealthBeat, 9/24).
- The federal health
reform law includes a little-noticed
provision that allocates $9 million annually
for four years, starting in 2010, for
programs to increase awareness about the
risk of breast cancer in women ages 15
through 44. Under the health reform
provision, CDC is charged with creating
educational campaigns focusing on breast
cancer in younger women and encouraging
healthy habits that promote prevention and
early detection. Groups that support young
women with breast cancer are eligible for
grants under the provision. The law also
directs NIH to develop new screening and
early-detection tests and prevention methods
for younger populations (Andrews,
Washington Post, 9/27).
Gearing Up for Midterm Elections
- Last week, Republicans
released their "Pledge to America," a
21-page document detailing how they would
limit the size of government -- in part by
repealing and replacing the federal health
reform law -- if they win a majority in the
midterm elections (Kane/Bacon,
Washington Post, 9/23). The
pledge states that the GOP would replace the
current overhaul with smaller measures, such
as ones to limit malpractice lawsuits
against physicians and enroll
individuals with chronic health conditions
in state-run high-risk insurance pools
(Bacon,
Washington Post, 9/23).
- Despite speculation
that Democrats are avoiding the subject of
the federal health reform law during
campaigning for midterm elections, several
House Democrats are putting the overhaul at
the forefront of their campaigns. Several
Democrats, including Reps. Shelly Berkley
(D-Nev.) and Dina Titus (D-Nev.), are
scheduling speeches alongside HHS Secretary
Kathleen Sebelius to address provisions in
the so-called "Patient's Bill of Rights"
that took effect last week. In addition,
some House Democrats are airing television
advertisements and writing opinion pieces in
their local newspapers to show their support
of the law (Haberkorn,
Politico,
9/27).
In
Public Opinion
- More than half of U.S.
residents incorrectly believe the federal
health reform law will raise their income
taxes and about one-quarter think the
overhaul includes so-called "death panels,"
according to a
recent Associated Press survey.
Among survey respondents who identified as
Republicans, accurate knowledge of the law
mattered little in their overall opposition
to it. Among Democrats and independents, the
poll found that respondents who were more
knowledgeable about the overhaul were more
likely to be in favor of it (Alonso-Zaldivar/Tompson,
AP/Miami Herald, 9/22).
- Another
recent Associated Press poll
found that many U.S. residents believe the
federal health care reform law did not
accomplish enough. The poll -- conducted by
Stanford University and funded by the Robert
Wood Johnson Foundation -- found that 30% of
Americans favor the overhaul, 40% oppose it
and 30% remain neutral. Four in 10 poll
respondents said that the health reform did
not do enough, regardless of their stance on
the law. Meanwhile, one in five said that
the government has no place being involved
in health care (Alonso-Zaldivar,
AP/Atlanta Journal-Constitution,
9/26).
Eye on
the Insurance Industry
- Insurers are
scrambling to adjust after the first
provisions of the federal health reform law
took effect last week. Some companies are
reducing administrative staff to lower
overhead costs, investing in technology
upgrades and training employees to expect a
surge in customer inquiries. In addition,
some insurers are altering their business
models to deal with the new rules. According
to some health experts, the adjustments
required under the health care overhaul
could put some insurers at risk of going out
of business (Abelson,
New York Times, 9/22).
- Many insurers are
facing the prospect of spending tens of
millions of dollars to overhaul their
coverage plans and reconfigure their
technological systems as they work to comply
with newly effective provisions of the
health reform law. The reform law now
requires insurers to fully cover the cost of
any preventive service, waive policyholders'
annual and lifetime spending limits and
accept all children, even those with
pre-existing conditions. In addition, some
insurers likely will cut costs to comply
with new medical-loss ratio rules (Sturdevant,
Hartford Courant, 9/24).
Read more:
http://www.californiahealthline.org/road-to-reform/2010/spotting-a-unicorn-acos-inch-closer-to-reality.aspx#ixzz11WpUdh2Z
ACCOUNTABLE CARE ORGANIZATIONS: New Rules
Soon... Very Soon
A proposal outlining the Obama
administration's preferred ground rules for new accountable care
organizations should be out within a month, says Donald M. Berwick,
administrator of the Centers for Medicare and Medicaid Services.
And Berwick signaled that he may fund other experiments in
coordination of care through the new Center for Medicare and Medicaid
Innovation.
The health care law, PPACA, (PL
111-148, PL 111-152) called for CM2
officials to fund a limited number of so-called accountable care
organizations (ACOs), which are groups of health care providers who
agree to be accountable for the quality, cost, and care of Medicare
recipients. The ACOs could take a variety of forms, such as networks
of physicians or partnerships between hospitals and physicians. These
new groups would test out the concept by agreeing to care for at least
5,000 people for three years or longer. If an ACO saved money, then
the medical providers who are part of the group would share in the
savings. Berwick declined to spell out what the proposed rule on
ACOs will say, but he acknowledged that federal officials will have to
sort through complicated and contentious issues.
"It's going to be tough," Berwick said.
Among the potential questions that
Berwick foresees:
-
How will the quality of care
for patients be measured? As Berwick noted, if measurements are
too stringent, then fewer providers will be interested in
participating.
-
How will antitrust laws be
relaxed so that providers can cooperate without being accused of
monopolistic behavior?
-
What kind of financial risk
will providers have to assume in order to form an ACO?
-
How can CM2
officials make sure that the ACOs
don't cherry-pick and recruit the healthiest patients to be part
of a group, leaving sicker patients out of the network?
-
How will patients be assigned
to an ACO? Berwick said that the "law
presumes choice," but it doesn't spell out the details
of how seniors can join or be assigned to an ACO.
When different medical groups join
together, how can providers make sure that they're protecting
patients' privacy?
How can small practices get the
capital to operate an ACO?
Berwick warned that he is looking
for proposals that will represent significant shifts in how patient
care is coordinated so that providers are really collaborating in a
new way that respects patients' preferences.
"Parties will be out there who will wish to
repackage the status quo. I don't think that will be enough,"
he said. "We're going to have to find a way
to deliver care better. That means change."
As Berwick searches for the best
models of coordinated care, the innovation center may separately fund
what he called "pioneering" organizations that began working on such
efforts without waiting for health law rules governing ACOs to be
written. Groups funded by the innovation center aren't expected to
have to adhere to the new ACO regulations.
Officials with the innovation
centerwhich has been operating for two months and funded four major
grants so farare in the midst of a 60-day strategic planning process.
Federal officials are coming up with a list of the type of projects
that they want to support through federal financing. In remarks to
reporters after the Brookings briefing, Berwick gushed about the
structure of the innovation center, saying that it
"allows us to move faster" than
officials can by using the rulemaking process and can
"invite reforms of exploration that wouldn't
be possible" otherwise.
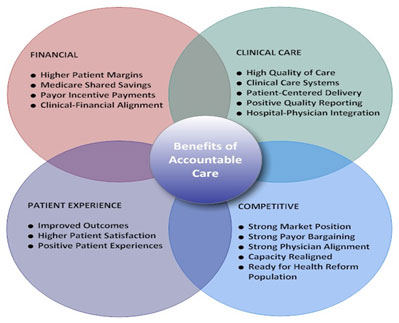
MINI-ME(D)
UPDATE: June 23,
2011: The Obama administration has announced
that it will shutting down a program that had
provided "Mini-Med" exemptions from the new
health care law for many employers and labor
unions offering bare-bones insurance coverage to
workers. No more applications will be accepted
after September 22, federal health officials
said. Steven B. Larsen, director of the federal
Center for Consumer Information and Insurance
Oversight, said employers and labor unions had
until that date to seek exemptions or request
the extension of waivers already granted. The
new health care law generally requires employers
to provide at least $750,000 in coverage to each
person in their health insurance plans this
year. Many restaurants, retailers and small
businesses do not meet the standard. Some
provide "mini-med" coverage with annual limits
that may be as low as $10,000.
Consider what it would be like to have a
health insurance plan that capped annual
benefits at $2,000. For any medical care costing
more than that, you would have to pay out of
pocket. Examples of care that costs more
than $2,000 and often a lot more include
virtually any
cancer treatment, any heart surgery, a
years worth of
diabetes treatment and care for many broken
bones. Even a single
M.R.I. exam
can cost more than $2,000. A typical
hospital stay runs thousands of dollars more.
So does this insurance plan sound like part of
the solution for the countrys health care
system or part of the problem?
A $2,000 plan happens to be one of the main
plans that
McDonalds offers its employees. It became
big news last week, when The Wall Street Journal
reported that
the company was worried the plan would run
afoul of a provision in the new health care law.
In response to the provision, McDonalds
threatened to drop the coverage altogether,
until the Obama
administration signaled it would grant some
exemptions.
This episode was only the latest disruption that
the health law seems to be causing. Also last
week, the
Principal Financial Group
said it was getting out of the health
insurance business, while other insurers have
said they might stop offering certain types of
coverage. With each new disruption come loud
claims some from insurance executives that
the health overhaul is damaging American health
care.
On the surface, these claims can sound credible.
But when you dig a little deeper, you often
discover the same lesson that the McDonalds
case provides: the real problem was the status
quo.
American families spend almost twice as much on
health care through premiums, paycheck
deductions and out-of-pocket expenses as
families in any other country. In exchange, we
receive top-notch specialty care in many areas.
Yet on the whole, we do not get much better care
than countries that spend far less.
We
dont live as long as people in Canada,
Japan, most of Western Europe or even relatively
poor Jordan.
Misdiagnosis is common.
Medical errors occur more often than in some
other countries. Unique to the developed world,
millions of people have no health insurance, and
millions more, like many fast-food workers,
are underinsured.
In choosing their health reform plan,
President Obama and the Democrats eschewed
radical changes,
for better or worse, and instead tried to
minimize the disruptions to the current system.
Sometimes, Mr. Obama went so far as to suggest
there would be no disruptions, saying that
people could keep their current plan if they
liked it. But thats not quite right. It is not
possible to change a system as huge, and as
hugely flawed, as ours without some disruptions.
McDonalds offers its hourly workers two
different health care plans, which are known as
mini-med plans. In one, workers can pay about
$730 a year for benefits of up to $2,000. In the
other, they can pay about $1,660 a year for
benefits of up to $10,000, The Journal reported.
In a memo to federal regulators, McDonalds
executives argued that their version of health
insurance positively impacts the almost 30,000
workers who are covered. And thats true. A plan
with a $2,000 or $10,000 cap can cover some
modest health problems and is better than being
uninsured.
But should the litmus test for American health
care really be better than nothing?
Mini-med plans force people to drain their
savings accounts for dozens of common medical
problems. They also force
hospitals to let some bills go unpaid, which
drives up costs for everyone else.
Senator
Charles Grassley, Republican of Iowa, has
previously criticized
AARP for marketing similarly limited plans
to its members. Its not better than nothing,
Mr. Grassley
argued, to encourage people to buy
something described as health security when
theres no basic protection against high medical
costs.
Dr. Aaron Carroll,
an
Indiana University
pediatrics professor who studies health
policy, says of mini-med plans: Theyre great
if youre healthy, because you feel like youre
covered. But if you ever need them, theyre so
skimpy, they provide very little. Gary Claxton
of the Kaiser Family Foundation adds, They
really just shouldnt be considered health
insurance.
The plans skimpiness is the main reason they
ran into legal jeopardy. Under the new law, most
plans must spend at least 85 percent of their
revenue on medical care, rather than
administrative overhead. The McDonalds plans
arent generous enough to clear the hurdle.
At the same time, its probably unrealistic to
expect McDonalds to give workers decent health
insurance. Many of those workers make less than
$20,000 a year.
A typical family insurance plan would raise
their total compensation by more than half,
destroying the McDonalds business model.
The workers, for their part, cannot afford to
buy insurance in the so-called individual
market. Plans are even more expensive in that
market, because it is dominated by people who
desperately need insurance which is to say,
sick people.
This is where health reform comes in. It tried
to solve the problem by creating what policy
experts call a three-legged stool.
First, people will be required to buy insurance,
to spread costs among the sick and the healthy.
Second, insurers will be prohibited from
cherry-picking only the healthiest customers,
again to spread costs. Finally, the government
will give subsidies to people, like McDonalds
workers, who cant afford insurance on their
own.
Germany, the Netherlands and Switzerland all use
a system along these lines to cover everyone,
largely through the private sector, for
less money per person than this country
spends.
The recent disruptions in our health insurance
market are partly a result of the fact that the
stools three legs were not built on the same
timetable. Some of the insurance regulations,
like the one on overhead costs, are starting to
take effect. But the new markets for health
insurance, known as exchanges, wont be up and
running until 2014. This timetable has its
problems, and the Obama administration will
probably need to grant some more temporary
exemptions.
In 2014, however, the choice for McDonalds
workers will no longer be between a bad policy
and no policy. Through the exchanges, they will
be able to buy a real health insurance plan
one that covers cancer, heart attacks,
surgeries, M.R.I.s and hospital stays. Dr.
Carroll notes that many families will end up
paying less than they are now paying out of
pocket and will get more access to care, too.
For insurance companies, these changes wont be
quite so positive. They will no longer be able
to sell plans that devote 30 percent of revenue
to salaries for their workers. They will not be
allowed to compete over which company can come
up with the most ingenious ways to say no to the
sick. Their benefits and prices will become more
public, thanks to the exchanges.
The health care overhaul that passed Congress is
far from ideal, as I
have written many
times in this space. But it does represent
progress.
The fact that it is beginning to disrupt the
status quo that some insurance policies will
eventually be eliminated and some inefficient
insurers will have to leave the market
altogether is all the proof we need.
back to
top
|




 Families USA Report:
"90 Million Uninsured at Some
Time During 2007-20079
Families USA Report:
"90 Million Uninsured at Some
Time During 2007-20079
 was going overseas. Almost all light assembly work was long gone and
heavy industries were moving production across the border. And
while, other economic factors contributed, a significant portion of
the blame laid at the foot of growing health insurance costs. Health
care was now 17.6% of the nation's economic market.
was going overseas. Almost all light assembly work was long gone and
heavy industries were moving production across the border. And
while, other economic factors contributed, a significant portion of
the blame laid at the foot of growing health insurance costs. Health
care was now 17.6% of the nation's economic market. Using
many of the same tactics that had derailed the Clinton health plan in
1994, a new Republican party emerged, the TeaParty/GOP. Fueled by
millions in newly "legalized" corporate PAC funds following a 5-4
Supreme Court decision in Citizens United v. Federal Election
Commission, 130 S.Ct. 876, January 10, 2010, and armed with ignorance,
the new TeaParty/GOP went on a crusade of lies and misrepresentations
about PPACA. Derisively labeling it as "Obamacare," the TeaParty/GOP
invented arguments against the law out of whole cloth, "death panels,"
"Obama's private army," "government takeover of health care,"
"bureaucrats controlling your health care." Using the Internet,
lying and factually-challenged e-mails went viral one after another.
Democrats congresscritters were confronted, and in some cases
physically assaulted, in their home districts when they tried to
explain the actual provision of the new law. Truth meant nothing.
Moderate Republicans faced a similar challenge and one after another,
they fell in primaries to the new TeaParty/GOPers. By the
November election, it was 1994 all over again, out went the Democrats
and in came the TeaParty/GOP and the well-tanned, well-rested Newt
Gingrich wanna-be clone, John Boehner. Their #1 promise, repeal
"Obamacare." It was déjà vu all over again.
Using
many of the same tactics that had derailed the Clinton health plan in
1994, a new Republican party emerged, the TeaParty/GOP. Fueled by
millions in newly "legalized" corporate PAC funds following a 5-4
Supreme Court decision in Citizens United v. Federal Election
Commission, 130 S.Ct. 876, January 10, 2010, and armed with ignorance,
the new TeaParty/GOP went on a crusade of lies and misrepresentations
about PPACA. Derisively labeling it as "Obamacare," the TeaParty/GOP
invented arguments against the law out of whole cloth, "death panels,"
"Obama's private army," "government takeover of health care,"
"bureaucrats controlling your health care." Using the Internet,
lying and factually-challenged e-mails went viral one after another.
Democrats congresscritters were confronted, and in some cases
physically assaulted, in their home districts when they tried to
explain the actual provision of the new law. Truth meant nothing.
Moderate Republicans faced a similar challenge and one after another,
they fell in primaries to the new TeaParty/GOPers. By the
November election, it was 1994 all over again, out went the Democrats
and in came the TeaParty/GOP and the well-tanned, well-rested Newt
Gingrich wanna-be clone, John Boehner. Their #1 promise, repeal
"Obamacare." It was déjà vu all over again. The
American Medical Association, American Hospital Association and
Pharmaceutical Research and Manufacturers of America are among many
groups that want to weaken or kill the
The
American Medical Association, American Hospital Association and
Pharmaceutical Research and Manufacturers of America are among many
groups that want to weaken or kill the